It is estimated that 47 million women go through menopause annually, and by 2030, 1.2 billion women will be post-menopausal. Hormone Replacement Therapy (HRT) is the medical standard of care in supporting women going through the transition and into their post menopause years. However, many women are opposed to HRT or have contraindications against using it [1]. This case report explores the implementation of a comprehensive dietary intervention and supplementation program to support a post-menopausal woman with promising outcomes as an alternative, natural therapy.
*Corresponding Author:
Sarah Doyle, DPT, CFMP, DACBN,
7 x Method, Miami Beach Florida, USA, Tel: 1-713-557-9987; Email:drsarah@drsarahdoyle.com
DOI: https://doi.org/10.1057/whr.2025.000029
ABSTRACT
It is estimated that 47 million women go through menopause annually, and by 2030, 1.2 billion women will be post-menopausal. Hormone Replacement Therapy (HRT) is the medical standard of care in supporting women going through the transition and into their post menopause years. However, many women are opposed to HRT or have contraindications against using it [1]. This case report explores the implementation of a comprehensive dietary intervention and supplementation program to support a post-menopausal woman with promising outcomes as an alternative, natural therapy.
Key words: Menopause, post menopause, estrogen, progesterone, hot flashes, weight gain, mood, depression, anxiety.
ABBREVIATIONS
HRT- Hormone Replacement Therapy
IBS – Irritable Bowel Syndrome
PCP – Primary Care Physician
DHEA – Dehydroepiandrosterone
SCN – Superchiasmatic nucleus
GABA – Gamma-aminobutyric acid
TCM – Traditional Chinese Medicine
EGCg – Epigallocatechin gallate
P5P – Pyridoxal 5 phosphate
SAMe – S-adenosyl – L – methionine
ATP – Adenosine triphosphate
CSF – Cerebrospinal fluid
INTRODUCTION
Fatigue, mood instability, weight gain, and sleep disturbances are common yet complex complaints for women midlife and beyond. These symptoms frequently coexist with conditions such as depression, hypertension, and hyperlipidemia, contributing to a diminished quality of life and motivating individuals to seek integrative or functional approaches to care [2]. Biohacking and lifestyle-based health optimization programs have gained popularity in recent years as patients search for alternatives to traditional pharmacologic treatments. Despite this growing interest, a limited body of published clinical data remains a shortcoming, describing patient experiences, outcomes, and successes within such programs.
This case report describes the experience of a 61-year-old female participant who entered a 12-week biohacking bootcamp with a broad constellation of symptoms, multiple chronic diagnoses, and significant dietary and lifestyle barriers. The menopausal transition is associated with hormonal fluctuations, metabolic dysregulation, and increased susceptibility to micronutrient insufficiencies, often exacerbating existing health concerns.
Through an integrative program combining targeted laboratory testing, individualized nutraceutical planning, nutrient-dense dietary strategies, circadian-aligned eating patterns, and weekly educational sessions, the participant demonstrated notable improvements in mood, metabolic markers, and functional capacity. Nutraceutical support was tailored to address hormonal regulation, stress-response pathways, and nutrient repletion based on clinical findings. Dietary support, aligned with circadian rhythm, was designed to support systemic inflammation and metabolic health.
This case highlights both the challenges and potential benefits of a structured integrative health program for women navigating the menopausal transition, offering insight into patient adherence, hormone-supportive strategies, and clinical outcomes over time.”
TIMELINE
2007
V.C. had a partial hysterectomy and was placed on HRT.
2018
V.C. was taken off HRT due to the risk of developing blood clots for an upcoming surgery.
2024-05-09
V.C. signed up for the 7X Method biohacking boot camp at a medical clinic with complaints of fatigue, joint pain, unintentional weight gain, mood swings, difficulty staying asleep, and a diagnosis of depression, hypertension, and irritable bowel syndrome (IBS).
2024-05-13
V.C. began the 7XMethod diet/lifestyle program.
2024-06-12
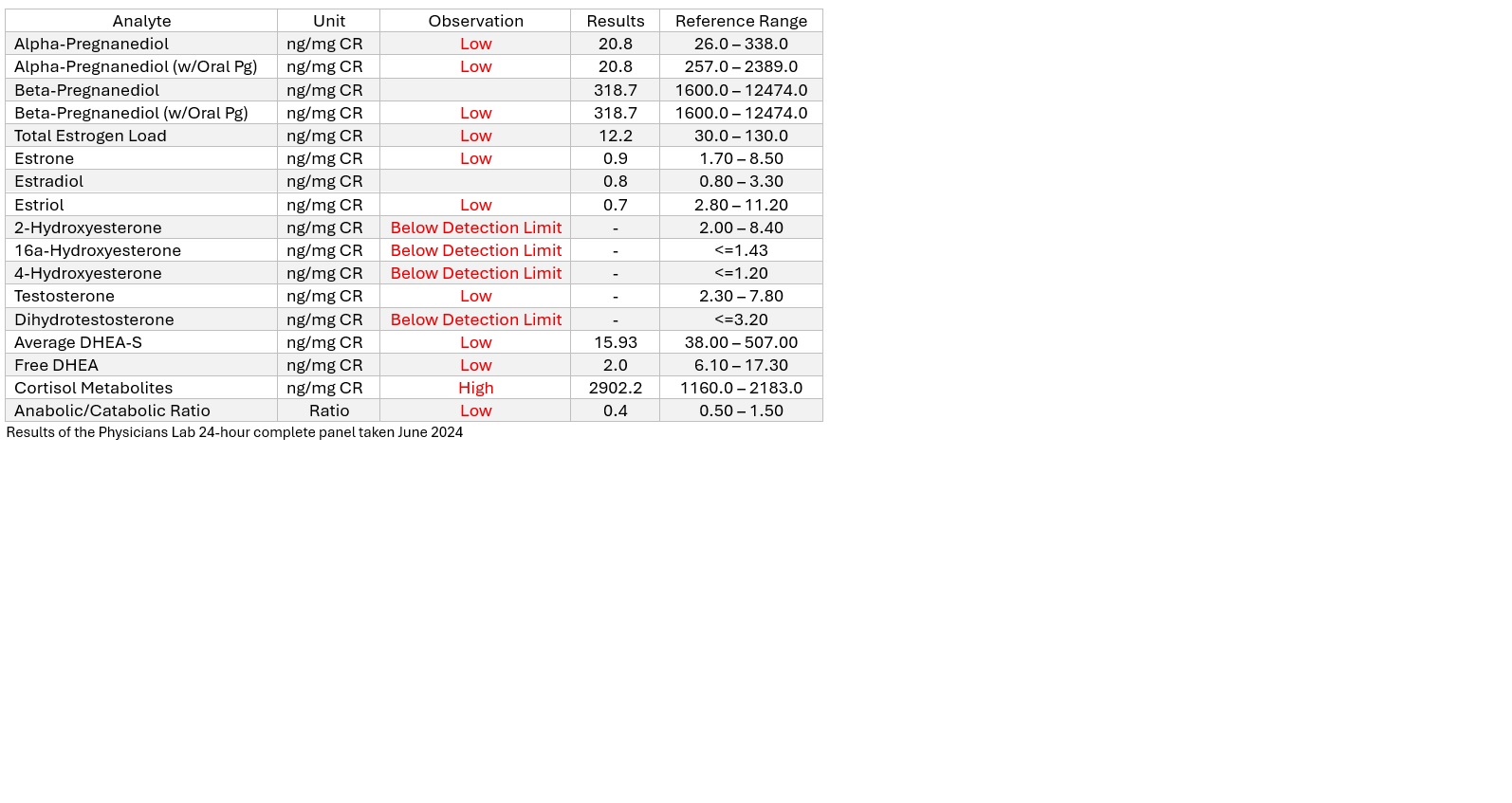
The Physicians Lab 24-hour comprehensive urine hormone panel test results were reviewed, and V.C. underwent a coaching session to discuss the test results, general recommendations, and supplement regimen.
2024-06-24
Supplements included: Designs for Health: (Complete Multi with Copper and Iron, SAMe, DopaBoost™, L-Glutamine, FemGuard + Balance™, LibidoStim-F™, Pregnenolone CRT™, and Amino Acid Synergy™) In addition with physician supervision, V.C. started weaning off Cymbalta.
2024-07-23
V.C. reported headaches that disrupted sleep as well as new-onset constipation, frequent crying spells, temper tantrums. Designs for Health 5-HTP Supreme™ for mental health support and magnesium malate as needed for constipation were recommended.
2024-08-05
V.C. started feeling “normal” and showed signs of mood improving.
2024-11-14
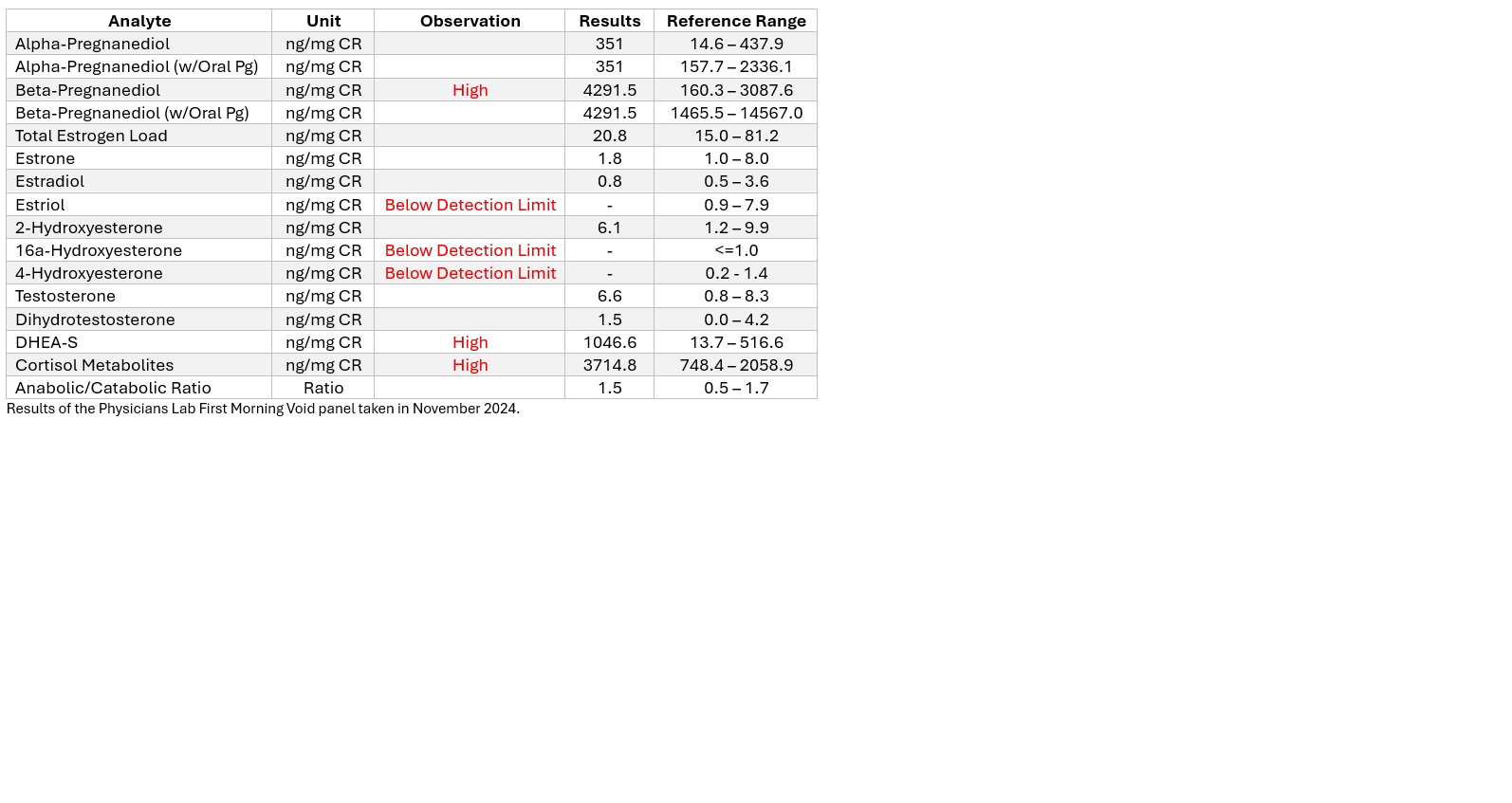
V.C. retested using the First Morning Void Profile by Physicians Lab to determine if there were improvements in hormone metabolites. Results indicated elevated DHEA, Beta Pregnanediol, but all the other analytes were in ideal ranges: Alpha Pregnanediol, Total Estrogen, Estradiol, and Testosterone – which indicated further improvement.
2025-05-11
A 12-month follow-up confirmed that V.C. was continuing to feel much better on the supplements than on the prescription SNRI. V.C. still complained of arthritic pain, although it was reported that V.C. was now able to get up and down off the floor; additionally, lower blood pressure was noted.
NARRATIVE
A 61-year-old female presented to a medical clinic to take part in the 7X Method biohacking bootcamp in May 2024. The patient (V.C.) presented with complaints of fatigue, joint pain, weight gain, mood swings, difficulty staying asleep, and depression. Additionally, V.C.'s Primary Care Physician (PCP) had diagnosed V.C. with IBS, depression, familial hypertension, and hyperlipidemia. V.C. has a desk job during the week and works as a waitress two nights per week. V.C. reported severe allergies to tree nuts and shellfish. V.C.’s overall eating habits are described as being “not very adventurous with food,” tending to be a picky eater, preferring very basic foods that “aren’t always the most nutritious.” V.C. had priorathletic prowess, playing softball three times per week until 45 years old. Despite maximum encouragement, V.C. is not currently exercising. V.C. was on hormone replacement therapy (HRT) between 2007 and 2018 after a partial hysterectomy. HRT was discontinued in 2018 as it was believed it was not safe to use HRT long-term, and concerns of an increased risk of blood clots for an upcoming surgery. V.C. started taking amlodipine for familial hypertension, starting in her early 30s. Cymbalta was prescribed for depression when V.C. was in their early 50s, and began taking Losartan in 2022 after their PCP noted elevated cholesterol.
The 7X Method bio hacking boot camp is a 12-weekprogram that includes a One-on-One telehealth consultations, as well as weekly group mastermind sessions covering topics such as the 7X Method, the gut-brain axis, women’s hormones, men’s hormones, nutrition education, cortisol, and sleep. The 7X Method bootcamp also included lab testing for thyroid, heavy metals, hormone metabolites, cortisol, methylation, and brain chemistry.
Via the Physicians Lab 24-hour comprehensive panel, V.C.’s hormone metabolites were tested in June of 2024. Follow-up testing in November 2024 utilized the Physicians Lab First Morning Void test. The 7X Method eating plan was initiated ahead of the delivery of the Physician’s Lab test kits. In this method, as outlined in the book 7X Method: The Truth About Food & Your Body That’s Never Been Told Until Now, the patient removed gluten and dairy from the diet and ate certain foods, at certain times of day, based on the circadian rhythm of the body's organs [Table 1].
Healthy fats like avocado, nuts, and coconut to support blood lipid levels were introduced. The patient was able to slowly integrate the dietary changes, taking a lot of steps outside her comfort zone. With these changes, V.C. reported losing 5.5 pounds between Monday (day 1) and Friday (day 5); by day 10, 6.6 pounds.
On June 12, 2024, the hormone metabolites test indicated low levels of progesterone, estrogen, and testosterone. At this point, the following nutraceuticals were incorporated: Designs for Health Complete Multi with Copper and Iron, SAMe, DopaBoost™, L-Glutamine, FemGuard + Balance™, LibidoStim-F™, Pregnenolone CRT™, and Amino Acid Synergy.
The patient started taking the supplements on June 24, 2024. Ultimately, V.C. discontinued taking the Complete Multi and Amino Acid Synergy™ after finishing the first complete cycle. On June 24, the patient also started to wean off Cymbalta with physician supervision; V.C. reported headaches that disrupted sleep as well as new-onset constipation. On July 23, 2024, the patient added Designs for Health 5-HTP Supreme™ to help stabilize her mood. Magnesium was also added, as needed for constipation.
On November 4th, the patient utilized the Physicians Lab First Morning Void test to determine if there were improvements in hormone metabolites. The patient reported compliance with all recommendations. V.C. had increased her intake of plant foods, following the rhythm outlined in the 7X Method, was avoiding dairy completely, had reduced gluten intake by 80%, and had remained consistent with the recommended supplement routine. In the follow-up testing, it was found that DHEA was elevated due to DHEA supplementation, but the patient did not report side effects of elevated DHEA, such as hirsutism, acne, oily skin, insomnia, hair thinning, or male-pattern baldness. The progesterone metabolite, Beta Pregnanediol, was slightly elevated, but all the other analytes were in ideal ranges: Alpha Pregnanediol, Total Estrogen, Estradiol, and Testosterone.
A 12-month follow-up confirmed that the patient was continuing tofeel much better on the nutraceutical regimen than on the prescription SNRI. V.C. still complained of arthritic pain in the knees and spine but also reported being able to get up and down off the floor, which V.C. was previously unable to do.
DIAGNOSTICS
Menopause occurs when a woman has not experienced a period for 12 consecutive months. A woman with an estrogen-deprived brain presents with semantic and verbal memory issues, decreased mental processing speed, mood fluctuations, impaired learning abilities, sleep disorders, fatigue, and hot flashes, among other things [2,3]. The patient had been in menopause for over a decade and presented with many textbook symptoms when beginning the biohacking bootcamp. Due to the symptoms presented, no differential diagnoses were considered in this case. The focus of the biohacking plan was to utilize education, nutrition via the 7X Method, and supplementation to support the patient's body, based on results from Physicians Lab testing. The coaching program opted for the Physicians Lab 24-Hour Comprehensive Profile, an at-home urine test that includes metabolites of progesterone, estrogen, androgens, and cortisol. The hormone metabolites indicated that the patient had high cortisol metabolites and low metabolites of progesterone, estrogen, testosterone, and dehydroepiandrosterone (DHEA). The 24-hour complete panel also analyzed the patient’s diurnal cortisol pattern. This indicated that overall cortisol output was elevated, but the cortisol pattern was in the normal range. Based on the results, there was a focus on raising progesterone, estrogen, and testosterone levels. No change in cortisol was needed [Table 2].
In November 2024, V.C. retested her hormone metabolites using the Physicians Lab First Morning Void Profile. This test was selected because the patient's diurnal cortisol pattern and overall cortisol output were within normal ranges in the 24-hour test taken in June 2024. The patient was instructed to collect the second morning void after taking her morning supplements to verify that the DHEA in the supplements was having an effect. The outcome was an increase in most estrogen metabolite markers, as well as progesterone and testosterone markers [Table 3].
DISCUSSION
Research In May 2025, there was a follow-up discussion to determine how the patient was feeling after one year of being on the recommended regimen. The patient confirmed that continuing with the supplementation and nutrition regimen, they continued to feel better than when they were taking Cymbalta. V.C. continued to experience arthritic pain in the knees and spine, but reported being able to get up and down off the floor, which was previously not possible. All the other symptoms the patient was initially feeling had also diminished. The patient also reported lower blood pressure since initiation of the biohacking bootcamp in 2024.
PATIENT PERSPECTIVE
1. What led you to seek care?
There were a few reasons but the biggest one for me was I wanted to get off of my prescription medication duloxetine.
2. How did you feel before, during, and after treatment?
I had a partial hysterectomy in 2007.Since then, I had been experiencing horrible menopause symptoms. Hot flashes, night sweats that were so bad I had to change my shirt. And the mood swings, and my memory. That was the scariest. I would drive down the road and forget where I was going, losing things, and forgetting appointments. I couldn't understand how I had such a sharp memory, I carried a 4.0 grade average, and now I can't remember what I had for dinner. And of course I was packing on weight. Then my PCP put me on the duloxetine. Every time I went to a doctor it was always the same excuse: it was because of my age or it was hereditary! Try this pill, cut back on that one. I didn't want to take any more pills. After I started taking the supplements, I'm not sure how I felt. I was having a real hard time coming off of the duloxetine. It was very hard, a lot and I mean a lot of crying. It felt hopeless. I was in a very dark place. Dr. Doyle really helped me through that rough spot. I think it was two weeks. That was really bad, and then it was like one day I woke up and I felt normal. I'm not sure what supplement or combination of supplements helped the memory. I have noticed that I can remember phone numbers again and I'm not as forgetful. I'm not as sharp as I was when I was 20 but there has been a noticeable improvement.
3. What changed for you emotionally physically or functionally?
I am much happier, I'm singing and laughing and joking like my old self. I DON'T HAVE ANY night sweats and on rare occasions I might get a hot flash but they are so few and far between and barely lasting a minute or two.
4. What has this process meant to you?
I'm not sure I can find the words to express what this whole process has meant to me. I'm quite pleased with all the results. I feel so much better and I'm thrilled about being able to recall details and phone numbers, etc.
5. Is there any advice or encouragement that you want to share with others?
Don't give up! Despite doctors telling you this is normal or age-related, there is an alternative and it sure as heck doesn't have to be a prescription.
DISCUSSION
Many women are opting for holistic options to support their bodies during the menopausal transition. For some, it does not want to use HRT; for others, they feel that HRT does not work well for their body, or they have contraindications for using HRT. A 2024 study on over 13,000 post-menopausal American women showed that HRT use had dropped from 26.9% in 1999 to 4.7% in 2020, among all age groups [1]. This is likely due to the controversial Women’s Health Initiative Clinical trial that was discontinued in 2004, which summarized that the risks outweighed the benefits when it came to hormone replacement therapy in menopausal women [4]. For this patient, HRT was used for several years but became a health risk. When symptoms returned, the patient sought holistic support.
The patient presented with typical menopause symptoms of vasomotor symptoms, sleep maintenance insomnia, decreased concentration, low energy, depression, and unintentional weight gain around the midsection and legs. The hormonal shifts that occur during the menopause transition increase the risk of developing cardiovascular disease, Type 2 diabetes, osteoporosis, and depression [3]. Cardiovascular disease is the leading cause of death for women in the U.S. Roughly 44% of women in the United States have cardiovascular disease, and roughly 1 in 5 women die from cardiovascular disease [5]. Estrogen is cardio protective in both men and women [6]. Decreased estrogen levels in a menopausal woman contribute to elevated triglycerides, visceral fat, and inflammation, even when a woman continues the diet and exercise regimen that kept her healthy in the decades preceding menopause [7]. In a meta-analysis of 22 studies, it was found that the development of depression and anxiety is common in women in the perimenopause to menopause transition [8]. Estrogen has been found to have neuroprotective effects, and with the erratic fluctuation and decline in estrogen during the menopausal transition, the neuroprotective effects are impacted [9]. Similar to estrogen, progesterone has a neuroprotective effect. It also acts as an anti-inflammatory and is protective against osteoporosis [10-12]. A randomized, double‑blind, placebo‑controlled clinical trial assessed the efficacy of pregnenolone supplementation in the presence of chronic low back pain in U.S. military veterans. The study hypothesized that metabolites of pregnenolone, such as allopregnanolone, would exhibit analgesic, anti‑inflammatory, and neuroprotective properties due to their Gamma-aminobutyric acid (GABA) receptor‑modulating actions [13]. After four weeks of pregnenolone administration, participants experienced a reduction in overall pain scores and a significant reduction in ratings of pain recall. More than 50% of individuals taking pregnenolone reported a 20% reduction in pain [13]. The study results also indicate that the treatment was safe and well‑tolerated [13]. Due to the low progesterone metabolites found in the Physicians Lab 24-Hour Comprehensive Profile, the symptoms indicating inflammation, and the patient’s diagnosis of depression, it was determined that pregnenolone would be beneficial for the patient. It was recommended that the patient take a double dose of Pregnenolone CRT™.
V.C. described her diet as consisting of simple foods with no green vegetable consumption. The 7X Method was implemented before supplementation to establish positive nutritional foundations and support her metabolic function, energy levels, and mental health. This way of eating centers on providing the organ systems in the body with specific types of energy at certain times of day, to work in harmony with the circadian rhythm of each organ system. Circadian rhythm is controlled by the suprachiasmatic nucleus (SCN) in the hypothalamus that acts as the body’s master clock. There are also synchronizing peripheral clocks in the organs and tissues in the body [14]. These peripheral clocks are governed by feedback loops guided by the SCN and drive hormonal metabolic rhythms [14]. In a review by Ribas-Latre and Eckel-Mahan (2016) they stated that nutrient input is also a primary driver of several peripheral clocks. The composition and the timing of a meal can disrupt peripheral clocks, even preventing synchronization with the master clock in the SCN [15]. Bautista et al (2025) stated that misalignment of circadian rhythms, whether due to genetic mutations, lifestyle factors or other factors, is recognized as a contributing factor to various pathologies, including metabolic syndrome, insulin resistance, and cardiovascular disease. As an example, in the 7X method, purple foods are recommended between 7-9 am to support DNA repair. Ribas-Latre and Eckel-Mahan (2016) state that foods which contain resveratrol, such as coffee, real dark chocolate or peanut butter feed SIRT1. SIRT1 plays a crucial role in controlling various key cellular functions, including DNA repair, cell death regulation, inflammation management, insulin secretion, mitochondrial production, and circadian rhythm maintenance [15]. Shifting to the 7XMethod, concentrating nutrition around the circadian rhythm helped V.C. to lose 5.5. lbs. in 5 days.
FemGuard + Balance™ was recommended at a standard dose of 4 capsules per day, divided. The blend of herbs and nutrients has been shown to support healthy hormonal balance and inflammatory response. Calcium‑D‑glucarate has been found to promote the proper elimination of excess estrogens through liver detoxification. Phase 1 liver metabolism involving cytochrome P450s makes toxins water-soluble. Phase 2 liver metabolisms involves conjugation with sulfates, glutathione, and glucuronic acid [1]. Calcium-D-glucarate can inhibit β-glucuronidase, allowing for more breakdowns of xenobiotics and xenoestrogens [16,17]. Diindolylmethane (DIM) is a metabolite of indole-3-carbinol that helps metabolize estrogens. If a woman’s detox pathway favors 16-OHE1 or 4-OHE1, DIM may assist in the metabolism of these. DIM has also been shown to improve 2-OHE1:16-OHE1 and 2-OHE1:4-OHE1 ratios, which can point to increased risk of breast cancer [16]. In addition to directly acting on estrogen metabolism, DIM has also been found to support a normal inflammatory response [18-20]. Black cohosh (Actaea racemose) is used to increase serotonin, which may help modulate hot flashes. In a placebo-controlled clinical trial, it was found that A. racemose contributed to reducing hot flashes and sweating in postmenopausal women [21]. Additionally, it helped to reduce sleep problems, irritability, and depressed mood when compared to the placebo group [21]. A 2020 study showed that black cohosh reduced C-reactive protein, low-density lipoprotein cholesterol, and triglycerides in menopausal women, which is significant if a woman has already begun developing signs or risk factors of cardiovascular disease that accompany a decrease in estrogen [2]. Chrysin is a dihydroxyflavone that exerts protective effects against estradiol-induced endometrial hyperplasia, a complex condition that occurs in postmenopausal women [22]. A study on post-ovariectomy rats showed chrysin had anxiolytic impact comparable to diazepam, suggesting chrysin can affect GABA receptors in surgically menopausal women [23]. Chaste tree berry (Vitex angus-castus) has been used to support menopause symptoms for thousands of years due to its estrogen boosting properties [2]. A 2019 double-blind, randomized control clinical trial with 52 subjects, 26 in the vitex group, 26 in the placebo group, found that the mean scores for menopausal disorder, vasomotor symptoms, and anxiety were significantly lower in the vitex group after eight weeks [24]. Vitex indirectly increases progesterone by reducing pituitary output of luteal phase prolactin [25-27]. Latent hyperprolactinemia due to insufficient dopamine inhibition of the pituitary can lead to cyclic mastalgia, where the patient experiences monthly breast tenderness. A systematic review concluded that vitex berry was found to ameliorate this [27,28].
LibidoStim-F™ is a blend of nutrients and botanicals to promote female sexual health and desire. The unique and targeted combination of ingredients provides support for natural testosterone production, optimization of testosterone and estrogen metabolism, healthy blood flow, and adrenal support. LibidoStim-F™ was recommended to the patient at a standard dose of 2 capsules per day to help support the patient’s sexual health, as well as hormone balance. A prospective randomized double-blind placebo-controlled trial using Tribulus terrestris concluded that T. terrestris has a positive impact in the domain of sexual interest and desire, arousal, and harmonious interaction with the partner, and comfort during sexual intercourse [29]. The bioactive steroidal saponins may help with healthy female libido by supporting the natural production of androgens and influencing nitric oxide release [30]. Horny goat weed (Epimedium) has been used in traditional Chinese medicine (TCM) for over 2000 years. It is known to support libido in both males and females, treating sexual dysfunction [31]. Additionally, it is shown to have protective effects against osteoporosis and offers support for menopause and PMS symptoms [31]. One clinical study found that horny goat weed can decrease lipids and increase estrogen for women in menopause without causing side effects [31]. In LibidoStim-F™, horny goat weed is standardized at 20% icariin. Icariin is a phytochemical flavonoid that is responsible for estrogen receptor-alpha selective estrogenic bioactivities [31]. Damiana (Turneradiffusa) has been used in Traditional medicine for its aphrodisiac properties in women. Its participation in the nitric oxide pathway accounts for the improvement in orgasm and lubrication [31]. Additionally, T. diffusa is a regulator of the natural balance between androgens and estrogen [32]. Reduced testosterone levels are related to decrease sexual activity in postmenopausal women [32]. Asian ginseng (Panax ginseng) acts in the Ishikawa cells of the endometrium as a competitive estrogen receptor-alpha and estrogen receptor-beta agonist [2]. Recent studies have shown P. ginseng to have antioxidant and anti-inflammatory effects in the aging brain [2]. A 2022 systematic review showed that ginseng had a positive effect on reducing hot flashes and menopause symptoms, and improved quality of life without affecting endometrial thickness, nor directly affecting sexual function, hormones, or biomarkers [33]. DHEA (dehydroepiandrosterone) is a naturally occurring compound in the body that is converted to estrogen and testosterone. Endogenous secretion of DHEA begins to decline in women around 30 years of age and becomes the only source of estrogen in postmenopausal women [34]. DHEA sulfate can increase the formation of pregnenolone by affecting steroid synthesis at the molecular level [35]. Reduced levels of estrogen can cause genitourinary syndrome of menopause [35]. This includes decreased tissue integrity within the bladder and urethra. The decreased tissue integrity can lead to vaginal microtears [35]. These microtears can cause pain during intimacy, which DHEA can help reduce [35,36]. One side effect of taking DHEA is that it can cause acne in some patients [36]. Tongkatali (Eurycomalongifolia), also known as Malaysian ginseng, is a safe, natural alternative to testosterone replacement therapy [37]. The testosterone support may help boost low libido levels. Ginkgo biloba extract has been shown to impart phytoestrogenic activity, increasing blood flow, and having a relaxing effect on smooth muscle tissue. In a placebo-controlled trial, it was shown that after 30 days of use, Ginkgo biloba significantly improved sexual desire in post-menopausal women [38].
DopaBoost™ was recommended to the patient to help V.C. achieve the goal of weaning off Cymbalta for depression. The patient was initially taking the recommended 2 capsules per day, but in September 2024, DopaBoost™ was discontinued and the dosage of 5HTP Supreme™ was doubled. DopaBoost™ is designed to support the body’s natural production of dopamine. Dopamine is essential for the normal functioning of the central nervous system, and it is associated with attention, learning, movement, balance, and mood regulation. The primary ingredient in DopaBoost™ is Mucuna pruriens, a botanical that naturally contains L-dopa, the metabolic precursor to dopamine, which can cross the blood-brain barrier. Additional ingredients include epigallocatechin gallate (EGCg), acetyl-L-tyrosine, quercetin, and vitamin B6, all selected for their synergistic roles in the production and regulation of dopamine.
5-HTP Supreme™ was recommended, in addition to DopaBoost™, to help the patient wean off Cymbalta. The patient began with 1 capsule per day along with DopaBoost™ but increased the dosage to 2 capsules per day in September 2024, because symptoms of depression were not improving. Although this paper is not focused on mental health or brain chemistry, it is important to note that estrogen withdrawal during menopause also affects the brain, causing decreased serotonin and norepinephrine production. Though this does account for hot flashes, night sweats, and difficulty sleeping, it can also present as depression and increased anxiety [30]. 5-HTP Supreme™ is a synergistic formula designed to support overall neurotransmitter metabolism by providing precursors of serotonin. 5‑hydroxytryptophan (5‑HTP) is a precursor to the biosynthesis of the neurotransmitter serotonin [39]. Due to its role in serotonin synthesis, 5‑HTP may be a supportive molecule for brain function and a healthy mood [39]. 5‑HTP is also a precursor to melatonin production, and it may also help support rapid eye movement (REM) stage sleep, increase sleep duration, and decrease sleep latency time [40]. A systematic review and meta‑analysis of clinical trials explored the potential efficacy of oral supplementation with 5‑HTP in individuals with depression [41]. The six studies that used the Hamilton Rating Scale for Depression (HAM‑D) reported average decreases of 12.70 points after supplementation with 5‑HTP [41]. On the HAM-D scale, a 12-point decrease in scores can indicate an improvement from severe depression to a healthy mental state [41]. Across studies included in this meta‑analysis, the effect for change in symptom severity was large, and most of the investigators reported high remission rates.41 Along with 5-HTP, 5-HTP Supreme™ contains Vitamin B6, pyridoxal 5‑phosphate (P5P). P5P is an essential cofactor to produce serotonin and its conversion to melatonin. Research indicates that P5P may support mood health, a normal stress response, and may support the synthesis of neurotransmitters to help support cognitive function and brain health. A cross‑sectional, population‑based survey aggregated data from 447 female adults regarding dietary intake of vitamins B6, B9, and B12. Dietary intake of vitamin B6 was shown to be associated with lower incidences of depression [42]. A meta-analysis and systematic review of 18 studies found inverse associations between depression and intake of dietary vitamin B6. The association was significant in females, but not in males [43].
S-adenosyl-L-methionine (SAMe) was also recommended to the patient, 1 capsule per day, to assist in reducing Cymbalta. SAMe is naturally synthesized from adenosine triphosphate (ATP) and methionine in the presence of cofactors folate and B12 [44]. SAMe is a methyl donor, meaning it helps facilitate chemical reactions that are crucial for neurotransmitter production and regulation, especially in the brain. SAMe plays a vital role in maintaining neuronal cellular membrane integrity and fluidity, which is critical for healthy neurotransmission and receptor function. Inadequate levels of SAMe in tissues, plasma, and cerebrospinal fluid (CSF), and/or the disturbance of transmethylation pathways are highly correlated with neurodegenerative and neuropsychiatric disorders, such as depression, Alzheimer's, and dementia [45]. There tends to be an increased demand for SAMe in people as they get older, if their diet does not support sufficient intake of methionine, B6, B12, and folate (vegetarian/vegan, poor protein intake).
L-Glutamine was recommended to the patient because it is known to support the health and function of intestinal mucosal cells. The patient’s recommended dose was 1 capsule of 850 mg per day. The amino acid L-glutamine is essential for the health of the immune system and the digestive tract. L-glutamine promotes the proliferation of enterocytes, helps regulate tight junction proteins, suppresses pro-inflammatory cytokine expression and signalling pathways, and protects against cellular stress [46]. In an eight-week, placebo-controlled study, it was found that in those with IBS-D and post-infectious hyperpermeability, L-glutamine dramatically reduced all IBS-D symptoms. Though the data is inconsistent, some women have an increase in IBS symptoms in post-menopause [47]. With the patient's IBS diagnosis, digestive support was recommended, especially with the change in diet and mental health support, either of which can cause a flare-up in IBS symptoms, as demonstrated by the increase in constipation upon reduction of the patient’s Cymbalta for depression.
LIMITATIONS
Research around the menopause transition relating tonutraceutical support and integrative nutrition is limited but growing. Limitations of this study are in part due to the limited amount of research available. Additionally, this case report outlines the outcomes of a single postmenopausal participant.The integrative approach included dietary modification, and nutraceutical supplementations were delivered concurrently. This makes it difficult to isolate the specific contribution of any single component. More research is needed to determine the efficacy of each component.
Conclusion
Dialogue around menopause is becoming more open and widespread. HRT has become part of that discussion, as an option to support a woman's body during the menopause transition. But for many, there are contraindications or a lingering fear of using HRT. For those who choose a more holistic route, they are seeking evidence-based information to support their decision.
This case highlights the effective application of an integrative nutrition model to address the multifactorial challenges in a 61-year-old female in post menopause. Within six months of the patient increasing the nutrient density of their diet, along with hormonal support via supplementation, the patient was able to improve her symptoms and improve her hormone metabolites. At-home urinary metabolite testing with nutraceutical supplementation provides a safe way to help manage menopause symptoms for women who do not have access to symptom management through their primary care provider.
ACKNOWLEDGEMENTS: This case report followed the CARE guidelines for case reports. Gratitude to Pamela K.B. Cho in support of writing this case report; and to Dr. Oscar Coetzee, a full professor at the Notre Dame of Maryland University, MD, and Danielle Arnold, an adjunct professor at Purdue Global University, for content review and reference updates. Also, thank you to Physicians Lab for providing the First Morning Void test used in November 2024.
FINANCIAL DISCLOSURES
No funding was received for the preparation and publication of this case report.
REFERENCES
1. Yang L, Toriola AT. Menopausal hormone therapy use among postmenopausal women. JAMA Health Forum. 2024; 5(9):e243128. doi:10.1001/jamahealthforum.2024.3128
2. Echeverria V, Echeverria F, Barreto GE, Echeverría J, Mendoza C. Estrogenic plants: to prevent neurodegeneration and memory loss and other symptoms in women after menopause. Front Pharmacol.2021; 12:644103. doi:10.3389/fphar.2021.644103
3. Silva GB, Pascucci JA, Karim H, et al. Influence of the onset of menopause on the risk of developing Alzheimer’s disease. Cureus. 2024; 16(9):e69124. doi:10.7759/cureus.69124
4. Thompson JJ, Ritenbaugh C, Nichter M. Why women choose compounded bioidentical hormone therapy: lessons from a qualitative study of menopausal decision-making. BMC Womens Health. 2017; 17(1):97. doi:10.1186/s12905-017-0449-0
5. CDC.gov. Heart disease: about women and heart disease. Centers for Disease Control. Updated May 15, 2024. https://www.cdc.gov/heart-disease/about/women-and-heart-disease.html
6. Nicholson CJ, Sweeney M, Robson SC, Taggart MJ. Estrogenic vascular effects are diminished by chronological aging. Sci Rep. 2017; 7:12153. doi:10.1038/s41598-017-12153-5
7. MešalićL, TupkovićE, KendićS, Balić D. Correlation between hormonal and lipid status in women in menopause. Bosn J Basic Med Sci. 2008; 8(2):188-192. doi:10.17305/bjbms.2008.2980
8. Bromberger JT, SchottL, Kravitz HM, Joffe H. Risk factors for major depression during midlife among a community sample of women with and without prior major depression: are they the same or different? Psychol Med. 2014; 45(8):1653-1664. doi:10.1017/s0033291714002773
9. Herson M, Kulkarni J. Hormonal agents for the treatment of depression associated with the menopause. DrugsAging. 2022; 39(8):607-618. doi:10.1007/s40266-022-00962-x
10. Cable JK, Grider MH. Physiology, progesterone. In: StatPearls. StatPearls Publishing. Updated May 1, 2023. https://www.ncbi.nlm.nih.gov/books/NBK558960/
11. Kaore SN, Langade DK, Yadav VK, Sharma P, Thawani VR, Sharma R. Novel actions of progesterone: what we know today and what will be the scenario in the future? J Pharm Pharmacol. 2012; 64(8):1040-1062. doi:10.1111/j.2042-7158.2012.01464.x
12. Fedotcheva TA, Fedotcheva NI, Shimanovsky NL. Progesterone as an anti-inflammatory drug and immunomodulator: new aspects in hormonal regulation of the inflammation. Biomolecules.2022; 12(9):1299. doi:10.3390/biom12091299
13. Naylor JC, Kilts JD, Shampine LJ, et al. Effect of pregnenolone vs placebo on self-reported chronic low back pain among US military veterans. JAMA Netw Open.2020; 3(3):e200287. doi:10.1001/jamanetworkopen.2020.0287
14. Bautista, J., Ojeda-Mosquera, S., Ordóñez-Lozada, D., & López-Cortés, A. (2025). Peripheral clocks and systemic zeitgeber interactions: from molecular mechanisms to circadian precision medicine. Frontiers in Endocrinology, 16. https://doi.org/10.3389/fendo.2025.1606242
15. Ribas-Latre, A., & Eckel-Mahan, K. (2016). Interdependence of nutrient metabolism and the circadian clock system: Importance for metabolic health. Molecular Metabolism, 5(3), 133–152. https://doi.org/10.1016/j.molmet.2015.12.006
16. Calcium-D-glucarate. Altern Med Rev.2002; 7(4):336-339.https://pubmed.ncbi.nlm.nih.gov/12197785/
17. Hanausek M, WalaszekZ, Slaga TJ. Detoxifying cancer causing agents to prevent cancer. Integr Cancer Ther. 2003; 2(2):139-144. doi:10.1177/1534735403002002005
18. Newman MS, SmeatonJ. The impact of 3,3’-diindolylmethane on estradiol and estrogen metabolism in postmenopausal women using a transdermal estradiol patch. Menopause. 2025; 32(7):630-639. doi:10.1097/gme.0000000000002542
19. Wu X, Liu J, Chen C, et al. 3,3’-diindolylmethane alleviates acute atopic dermatitis by regulating T cell differentiation in a mouse model. Mol Immunol. 2021; 130:104-112. doi:10.1016/j.molimm.2020.11.013.
20. Lee J. 3,3’-diindolylmethane inhibits TNF-α- and TGF-β-induced epithelial-mesenchymal transition in breast cancer cells. Nutr Cancer. 2019; 71(6):992-1006.
doi:10.1080/01635581.2019.1577979
21. Dietz BM, Hajirahimkhan A, Dunlap TL, Bolton JL. Botanicals and their bioactive phytochemicals for women’s health. Pharmacol Rev.2016; 68(4):1026-1073. doi.org/10.1124/pr.115.010843
22. Eid BG. Chrysin attenuates estradiol-induced endometrial hyperplasia in rats via enhancing PPARα activity. Environ Sci Pollut ResInt. 2022; 29(36):54273-54281. doi:10.1007/s11356-022-19206-x
23. Rodríguez-Landa JF, Hernández-López F, Cueto-Escobedo J, et al. Chrysin (5,7-dihydroxyflavone) exerts anxiolytic-like effects through GABAA receptors in a surgical menopause model in rats. BiomedPharmacother. 2018; 109:2387-2395. doi:10.1016/j.biopha.2018.11.111
24. Naseri R, Farnia V, Yazdchi K, Alikhani M, Basanj B, Salemi S. Comparison of Vitex agnus-castusextracts with placebo in reducing menopausal symptoms: a randomized double-blind study. Korean J Fam Med. 2019; 40(6):362-367. doi:10.4082/kjfm.18.0067
25. Milewicz A, Gejdel E, Sworen H, Sienkiewicz K, Jedrzejak J, Teucher T, Schmitz H. Vitex agnus castus extract in the treatment of luteal phase defects due to latent hyperprolactinemia. Results of a randomized placebo-controlled double-blind study [German.] Arzneimittelforschung. 1993:43(7):752-756. PMID: 8369008.
26. Van DieM, Burger H, Teede H, Bone K. Vitex agnus-castusextracts for female reproductive disorders: a systematic review of clinical trials. Planta Medica, 2012; 79(07):562-575. doi:10.1055/s-0032-1327831
27. Shaw S, Wyatt K, Campbell J, ErnstE, Thompson-Coon J. Vitex agnus castus for premenstrual syndrome. Cochrane Database System Rev.2018; 2018(3):CD004632. doi:10.1002/14651858.cd004632.pub2
28. Ooi SL, Watts S, McClean R, Pak SC. Vitex agnus-castus for the treatment of cyclic mastalgia: a systematic review and meta-analysis. J Womens Health. 2019; 29(2):262-278. doi:/10.1089/jwh.2019.7770
29. Lima S, Yamada S, Reis B, Silva G, Aoki T, Postigo S. Assessment of the effects of Tribulus terrestris on sexual function of menopausal women. Rev Bras Ginecol Obstet. 2016; 38(03):140-146. doi:10.1055/s-0036-1571472
30. Sahin K, Orhan C, Akdemir F, et al. Comparative evaluation of the sexual functions and NF-κB and Nrf2 pathways of some aphrodisiac herbal extracts in male rats. BMC ComplementAltern Med. 2016; 16(1):318. doi:10.1186/s12906-016-1303-x
31. Estrada-Reyes R, Carro-Juárez M, Martínez-Mota L. Pro-sexual effects of Turneradiffusa Wild (Turneraceae) in male rats involves the nitric oxide pathway. JEthnopharmacol. 2013; 146(1):164-172. doi:10.1016/j.jep.2012.12.025
32. PalaciosS, Soler E, Ramírez M, Lilue M, Khorsandi D, Losa F. Effect of a multi-ingredient based food supplement on sexual function in women with low sexual desire. BMC Womens Health. 2019; 19(1):58. doi:10.1186/s12905-019-0755-9
33. Lee HW, Ang L,Lee MS. Using ginseng for menopausal women’s health care: a systematic review of randomized placebo-controlled trials. Complement Ther Clin Pract. 2022; 48:101615. doi:10.1016/j.ctcp.2022.101615
34. Labrie F, Bélanger A, Pelletier G, Martel C, Archer DF, Utian WH. Science of intracrinology in postmenopausal women. Menopause. 2017; 24(6):702-712. doi:10.1097/gme.0000000000000808
35. Neunzig J, Bernhardt R. Dehydroepiandrosterone sulfate (DHEAS) stimulates the first step in the biosynthesis of steroid hormones. PLoS One, 2014; 9(2):e89727. doi:10.1371/journal.pone.0089727
36. Scheffers CS, ArmstrongS., Cantineau AE, Farquhar C, JordanV. Dehydroepiandrosterone for women in the peri- or postmenopausal phase.Cochrane Database Syst Rev. 2015; 1(1):CD011066. doi:10.1002/14651858.cd011066.pub2
37. George A, Henkel R. Phytoandrogenic properties of Eurycomalongifoliaas natural alternative to testosterone replacement therapy. Andrologia. 2014; 46(7):708-721. doi:10.1111/and.12214
38. Pebdani MA, Taavoni S, Seyedfatemi N, Haghani H. Triple-blind, placebo-controlled trial of Ginkgo biloba extract on sexual desire in postmenopausal women in Tehran.Iran J Nurs Midwifery Res. 2014; 19(3):262-265. https://pmc.ncbi.nlm.nih.gov/articles/PMC4061626/
39. Maffei ME. 5-Hydroxytryptophan (5-HTP): natural occurrence, analysis, biosynthesis, biotechnology, physiology and toxicology. Int JMolecular Sci. 2020; 22(1):181. doi:10.3390/ijms22010181
40. Kwon JI, Park Y, Han SH, Suh HJ. Hydrolysate preparation with high content of 5-hydroxytryptophan from liquid egg protein and its sleep-potentiating activity. Korean J Food Sci Anim Resour. 2017; 37(5):646-653. doi:10.5851/kosfa.2017.37.5.646
41. Javelle F, Lampit A, Bloch W, Häussermann P, Johnson SL, Zimmer P. Effects of 5 hydroxytryptophan on distinct types of depression: a systematic review and meta analysis. Nutr Rev. 2020; 78(1):77 88. doi:10.1093/nutrit/nuz039.
42. Mozaffari H, DarooghegiMofrad M, Surkan PJ, Askari M, Azadbakht L. Associations between dietary intake of B vitamins and psychological disorders among Iranian women: a cross sectional study. Public Health Nutr. 2021; 24(7):1787 1797. doi:10.1017/S1368980020002943.
43. Wu Y, Zhang L, Li S, Zhang D. Associations of dietary vitamin B1, vitamin B2, vitamin B6, and vitamin B12 with the risk of depression: a systematic review and meta-analysis. Nutr Rev. 2021; 80(3):351-366. doi:10.1093/nutrit/nuab014
44. Ouyang Y, Wu Q, Li J, Sun S, Sun S. S‐adenosylmethionine: a metabolite critical to the regulation of autophagy. Cell Prolif. 2020; 53(11):e12891. doi:10.1111/cpr.12891rg/10.1007/s13311-017-0593-0
46. Kim M, Kim H. The roles of glutamine in the intestine and its implication in intestinal diseases. Int J MolecularSci. 2017; 18(5):1051. doi:10.3390/ijms18051051
47. Olafsdottir LB, Gudjonsson H, Jonsdottir HH, Björnsson E, Thjodleifsson B. Natural history of irritable bowel syndrome in women and dysmenorrhea: a 10-year follow-up study. Gastroenterol Res Pract.2012; 2012:1-7. doi:10.1155/2012/534204
PEER REVIEW
Not commissioned. Externally peer reviewed.


1. Yang L, Toriola AT. Menopausal hormone therapy use among postmenopausal women. JAMA Health Forum. 2024; 5(9):e243128. doi:10.1001/jamahealthforum.2024.3128
2. Echeverria V, Echeverria F, Barreto GE, Echeverría J, Mendoza C. Estrogenic plants: to prevent neurodegeneration and memory loss and other symptoms in women after menopause. Front Pharmacol.2021; 12:644103. doi:10.3389/fphar.2021.644103
3. Silva GB, Pascucci JA, Karim H, et al. Influence of the onset of menopause on the risk of developing Alzheimer’s disease. Cureus. 2024; 16(9):e69124. doi:10.7759/cureus.69124
4. Thompson JJ, Ritenbaugh C, Nichter M. Why women choose compounded bioidentical hormone therapy: lessons from a qualitative study of menopausal decision-making. BMC Womens Health. 2017; 17(1):97. doi:10.1186/s12905-017-0449-0
5. CDC.gov. Heart disease: about women and heart disease. Centers for Disease Control. Updated May 15, 2024. https://www.cdc.gov/heart-disease/about/women-and-heart-disease.html
6. Nicholson CJ, Sweeney M, Robson SC, Taggart MJ. Estrogenic vascular effects are diminished by chronological aging. Sci Rep. 2017; 7:12153. doi:10.1038/s41598-017-12153-5
7. MešalićL, TupkovićE, KendićS, Balić D. Correlation between hormonal and lipid status in women in menopause. Bosn J Basic Med Sci. 2008; 8(2):188-192. doi:10.17305/bjbms.2008.2980
8. Bromberger JT, SchottL, Kravitz HM, Joffe H. Risk factors for major depression during midlife among a community sample of women with and without prior major depression: are they the same or different? Psychol Med. 2014; 45(8):1653-1664. doi:10.1017/s0033291714002773
9. Herson M, Kulkarni J. Hormonal agents for the treatment of depression associated with the menopause. DrugsAging. 2022; 39(8):607-618. doi:10.1007/s40266-022-00962-x
10. Cable JK, Grider MH. Physiology, progesterone. In: StatPearls. StatPearls Publishing. Updated May 1, 2023. https://www.ncbi.nlm.nih.gov/books/NBK558960/
11. Kaore SN, Langade DK, Yadav VK, Sharma P, Thawani VR, Sharma R. Novel actions of progesterone: what we know today and what will be the scenario in the future? J Pharm Pharmacol. 2012; 64(8):1040-1062. doi:10.1111/j.2042-7158.2012.01464.x
12. Fedotcheva TA, Fedotcheva NI, Shimanovsky NL. Progesterone as an anti-inflammatory drug and immunomodulator: new aspects in hormonal regulation of the inflammation. Biomolecules.2022; 12(9):1299. doi:10.3390/biom12091299
13. Naylor JC, Kilts JD, Shampine LJ, et al. Effect of pregnenolone vs placebo on self-reported chronic low back pain among US military veterans. JAMA Netw Open.2020; 3(3):e200287. doi:10.1001/jamanetworkopen.2020.0287
14. Bautista, J., Ojeda-Mosquera, S., Ordóñez-Lozada, D., & López-Cortés, A. (2025). Peripheral clocks and systemic zeitgeber interactions: from molecular mechanisms to circadian precision medicine. Frontiers in Endocrinology, 16. https://doi.org/10.3389/fendo.2025.1606242
15. Ribas-Latre, A., & Eckel-Mahan, K. (2016). Interdependence of nutrient metabolism and the circadian clock system: Importance for metabolic health. Molecular Metabolism, 5(3), 133–152. https://doi.org/10.1016/j.molmet.2015.12.006
16. Calcium-D-glucarate. Altern Med Rev.2002; 7(4):336-339.https://pubmed.ncbi.nlm.nih.gov/12197785/
17. Hanausek M, WalaszekZ, Slaga TJ. Detoxifying cancer causing agents to prevent cancer. Integr Cancer Ther. 2003; 2(2):139-144. doi:10.1177/1534735403002002005
18. Newman MS, Smeaton J. The impact of 3,3’-diindolylmethane on estradiol and estrogen metabolism in postmenopausal women using a transdermal estradiol patch. Menopause. 2025; 32(7):630-639. doi:10.1097/gme.0000000000002542
19. Wu X, Liu J, Chen C, et al. 3,3’-diindolylmethane alleviates acute atopic dermatitis by regulating T cell differentiation in a mouse model. Mol Immunol. 2021; 130:104-112. doi:10.1016/j.molimm.2020.11.013.
20. Lee J. 3,3’-diindolylmethane inhibits TNF-α- and TGF-β-induced epithelial-mesenchymal transition in breast cancer cells. Nutr Cancer. 2019; 71(6):992-1006.
doi:10.1080/01635581.2019.1577979
21. Dietz BM, Hajirahimkhan A, Dunlap TL, Bolton JL. Botanicals and their bioactive phytochemicals for women’s health. Pharmacol Rev.2016; 68(4):1026-1073. doi.org/10.1124/pr.115.010843
22. Eid BG. Chrysin attenuates estradiol-induced endometrial hyperplasia in rats via enhancing PPARα activity. Environ Sci Pollut ResInt. 2022; 29(36):54273-54281. doi:10.1007/s11356-022-19206-x
23. Rodríguez-Landa JF, Hernández-López F, Cueto-Escobedo J, et al. Chrysin (5,7-dihydroxyflavone) exerts anxiolytic-like effects through GABAA receptors in a surgical menopause model in rats. BiomedPharmacother. 2018; 109:2387-2395. doi:10.1016/j.biopha.2018.11.111
24. Naseri R, Farnia V, Yazdchi K, Alikhani M, Basanj B, Salemi S. Comparison of Vitex agnus-castusextracts with placebo in reducing menopausal symptoms: a randomized double-blind study. Korean J Fam Med. 2019; 40(6):362-367. doi:10.4082/kjfm.18.0067
25. Milewicz A, Gejdel E, Sworen H, Sienkiewicz K, Jedrzejak J, Teucher T, Schmitz H. Vitex agnus castus extract in the treatment of luteal phase defects due to latent hyperprolactinemia. Results of a randomized placebo-controlled double-blind study [German.] Arzneimittelforschung. 1993:43(7):752-756. PMID: 8369008.
26. Van DieM, Burger H, Teede H, Bone K. Vitex agnus-castusextracts for female reproductive disorders: a systematic review of clinical trials. Planta Medica, 2012; 79(07):562-575. doi:10.1055/s-0032-1327831
27. Shaw S, Wyatt K, Campbell J, ErnstE, Thompson-Coon J. Vitex agnus castus for premenstrual syndrome. Cochrane Database System Rev.2018; 2018(3):CD004632. doi:10.1002/14651858.cd004632.pub2
28. Ooi SL, Watts S, McClean R, Pak SC. Vitex agnus-castus for the treatment of cyclic mastalgia: a systematic review and meta-analysis. J Womens Health. 2019; 29(2):262-278. doi:/10.1089/jwh.2019.7770
29. Lima S, Yamada S, Reis B, Silva G, Aoki T, Postigo S. Assessment of the effects of Tribulus terrestris on sexual function of menopausal women. Rev Bras Ginecol Obstet. 2016; 38(03):140-146. doi:10.1055/s-0036-1571472
30. Sahin K, Orhan C, Akdemir F, et al. Comparative evaluation of the sexual functions and NF-κB and Nrf2 pathways of some aphrodisiac herbal extracts in male rats. BMC ComplementAltern Med. 2016; 16(1):318. doi:10.1186/s12906-016-1303-x
31. Estrada-Reyes R, Carro-Juárez M, Martínez-Mota L. Pro-sexual effects of Turneradiffusa Wild (Turneraceae) in male rats involves the nitric oxide pathway. JEthnopharmacol. 2013; 146(1):164-172. doi:10.1016/j.jep.2012.12.025
32. PalaciosS, Soler E, Ramírez M, Lilue M, Khorsandi D, Losa F. Effect of a multi-ingredient based food supplement on sexual function in women with low sexual desire. BMC Womens Health. 2019; 19(1):58. doi:10.1186/s12905-019-0755-9
33. Lee HW, Ang L,Lee MS. Using ginseng for menopausal women’s health care: a systematic review of randomized placebo-controlled trials. Complement Ther Clin Pract. 2022; 48:101615. doi:10.1016/j.ctcp.2022.101615
34. Labrie F, Bélanger A, Pelletier G, Martel C, Archer DF, Utian WH. Science of intracrinology in postmenopausal women. Menopause. 2017; 24(6):702-712. doi:10.1097/gme.0000000000000808
35. Neunzig J, Bernhardt R. Dehydroepiandrosterone sulfate (DHEAS) stimulates the first step in the biosynthesis of steroid hormones. PLoS One, 2014; 9(2):e89727. doi:10.1371/journal.pone.0089727
36. Scheffers CS, ArmstrongS., Cantineau AE, Farquhar C, JordanV. Dehydroepiandrosterone for women in the peri- or postmenopausal phase.Cochrane Database Syst Rev. 2015; 1(1):CD011066. doi:10.1002/14651858.cd011066.pub2
37. George A, Henkel R. Phytoandrogenic properties of Eurycomalongifoliaas natural alternative to testosterone replacement therapy. Andrologia. 2014; 46(7):708-721. doi:10.1111/and.12214
38. Pebdani MA, Taavoni S, Seyedfatemi N, Haghani H. Triple-blind, placebo-controlled trial of Ginkgo biloba extract on sexual desire in postmenopausal women in Tehran.Iran J Nurs Midwifery Res. 2014; 19(3):262-265. https://pmc.ncbi.nlm.nih.gov/articles/PMC4061626/
39. Maffei ME. 5-Hydroxytryptophan (5-HTP): natural occurrence, analysis, biosynthesis, biotechnology, physiology and toxicology. Int JMolecular Sci. 2020; 22(1):181. doi:10.3390/ijms22010181
40. Kwon JI, Park Y, Han SH, Suh HJ. Hydrolysate preparation with high content of 5-hydroxytryptophan from liquid egg protein and its sleep-potentiating activity. Korean J Food Sci Anim Resour. 2017; 37(5):646-653. doi:10.5851/kosfa.2017.37.5.646
41. Javelle F, Lampit A, Bloch W, Häussermann P, Johnson SL, Zimmer P. Effects of 5 hydroxytryptophan on distinct types of depression: a systematic review and meta analysis. Nutr Rev. 2020; 78(1):77 88. doi:10.1093/nutrit/nuz039.
42. Mozaffari H, DarooghegiMofrad M, Surkan PJ, Askari M, Azadbakht L. Associations between dietary intake of B vitamins and psychological disorders among Iranian women: a cross sectional study. Public Health Nutr. 2021; 24(7):1787 1797. doi:10.1017/S1368980020002943.
43. Wu Y, Zhang L, Li S, Zhang D. Associations of dietary vitamin B1, vitamin B2, vitamin B6, and vitamin B12 with the risk of depression: a systematic review and meta-analysis. Nutr Rev. 2021; 80(3):351-366. doi:10.1093/nutrit/nuab014
44. Ouyang Y, Wu Q, Li J, Sun S, Sun S. S‐adenosylmethionine: a metabolite critical to the regulation of autophagy. Cell Prolif. 2020; 53(11):e12891. doi:10.1111/cpr.12891rg/10.1007/s13311-017-0593-0
46. Kim M, Kim H. The roles of glutamine in the intestine and its implication in intestinal diseases. Int J MolecularSci. 2017; 18(5):1051. doi:10.3390/ijms18051051
47. Olafsdottir LB, Gudjonsson H, Jonsdottir HH, Björnsson E, Thjodleifsson B. Natural history of irritable bowel syndrome in women and dysmenorrhea: a 10-year follow-up study. Gastroenterol Res Pract.2012; 2012:1-7. doi:10.1155/2012/534204
The Roles of Choline in Maintaining Optimal Health
The Effects of Intake of Bread with Treated Corn Bran Inclusion on Postprandial Glyceamic Response
Food Waste throughout the Food Production Continuum – Water Food and Energy Nexus
Use of Lightly Potassium-Enriched Soy Sauce at Home Reduced Urinary Sodium-to-Potassium Ratio
A Different Type of Critical Migration
PRECEDE: A Conceptual Model to Assess Immigrant Health
Walking Together: Supporting Indigenous Student Success in University
Cosmetic Surgery and Body Image in Race/Ethnic Minorities
Our articles most useful
Beth Turner, Charlotte Garrett and Anja Wittkowski
Published : February 13, 2018
Women's Health Research
Yinjia Guo, Min Zhao, Victoria Rutten, Yifei Gao, Arier Lee, Qi Chen
Published : November 22, 2017
Women's Health Research
Jessi Hanson-DeFusco*
Published : December 07, 2023
Women's Health Research
Dana R. Riedy, Sarah M. Ghose, Sahar M. Sabet, Morgan P. Reid, Claire M. Williams, Ashley MacPherson and Natalie D. Dautovich
Published : October 11, 2023
Women's Health Research
Peggy B. Smith MA*, Reginald Hatter, Jasmine King, Anne Van Horn and Sophie McCollum
Published : November 16, 2023
Women's Health Research
Shanette M. Harris
Published : August 22, 2022
Women's Health Research