Objectives: Assess categorisation of urgency of cesarean section in UK following NICE guidelines (2011).
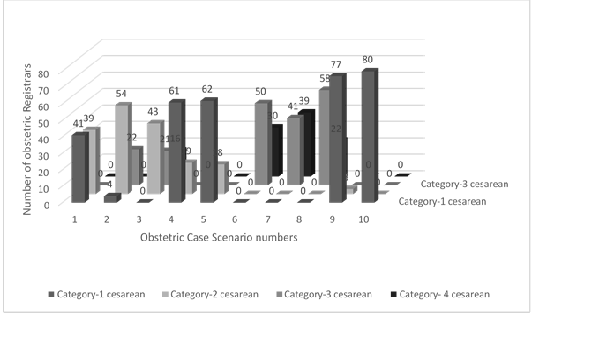
Design: Cross-sectional survey of 80 obstetric registrars from different regions using a questionnaire to categorise 10 scenarios into four-category urgency of cesareans.
Results: Wide variation was seen with up to 25 -50% discordance for all categories, importantly affecting categories 1 and 2, a significant concern expressed by NICE in 2011. Almost all stated that decision-to-delivery-interval (DDI) for category-1 cesareans should be 30 minutes as opposed to “as soon as possible” (endeavour for 15 minutes) specified by NICE. Most registrars classed “conventional” fetal distress (no immediate threat to fetus) also into category-1, jumbled with very urgent (crash) cesareans. The Registrars commented they felt confused and dissatisfied with the current practice of categorisation.
Conclusions: This study demonstrates that the four-category classification of cesareans is very inconsistent in actual practice. The main impetus behind this categorisation was to remove the entrenched arbitrary 30minute DDI standard for cases of fetal distress by placing them in category-2. But the NICE recommendation of DDI of less than 75 minutes (level 3 evidence) for category-2 has unintended consequence making obstetricians feel uncomfortable and thereby class these as category-1. This also dilutes the recommended DDI for category-1 which should include only very urgent (crash) cesareans generally associated with acute hypoxic events like cord-prolapse. Although it would be possible to muddle along with dysfunctional practice, this study identifies the need, areas and essential solutions for improvement. The guideline-groups should recommend a more pragmatic range of DDI of 40-50 minutes or so (achievable without undue distress to mothers or excessive demands on service) for category-2 cesareans. Recommended optimal DDI should not be confused with more liberal audit standards as apparent in this study. Simply highlighting a continuous spectrum of time-frames to be individualised for each case doesn’t seem to be working. More explicit and definitive guidance by giving multiple examples of each category with particular focus on cases of conventional fetal distress (category-2) as described in this paper seems necessary if satisfactory standardisation of practice is to be achieved for meaningful data collection, audits and research.
Our articles most useful
Beth Turner, Charlotte Garrett and Anja Wittkowski
Published : February 13, 2018
Women's Health Research
Yinjia Guo, Min Zhao, Victoria Rutten, Yifei Gao, Arier Lee, Qi Chen
Published : November 22, 2017
Women's Health Research
Jessi Hanson-DeFusco*
Published : December 07, 2023
Women's Health Research
Dana R. Riedy, Sarah M. Ghose, Sahar M. Sabet, Morgan P. Reid, Claire M. Williams, Ashley MacPherson and Natalie D. Dautovich
Published : October 11, 2023
Women's Health Research
Peggy B. Smith MA*, Reginald Hatter, Jasmine King, Anne Van Horn and Sophie McCollum
Published : November 16, 2023
Women's Health Research
Shanette M. Harris
Published : August 22, 2022
Women's Health Research