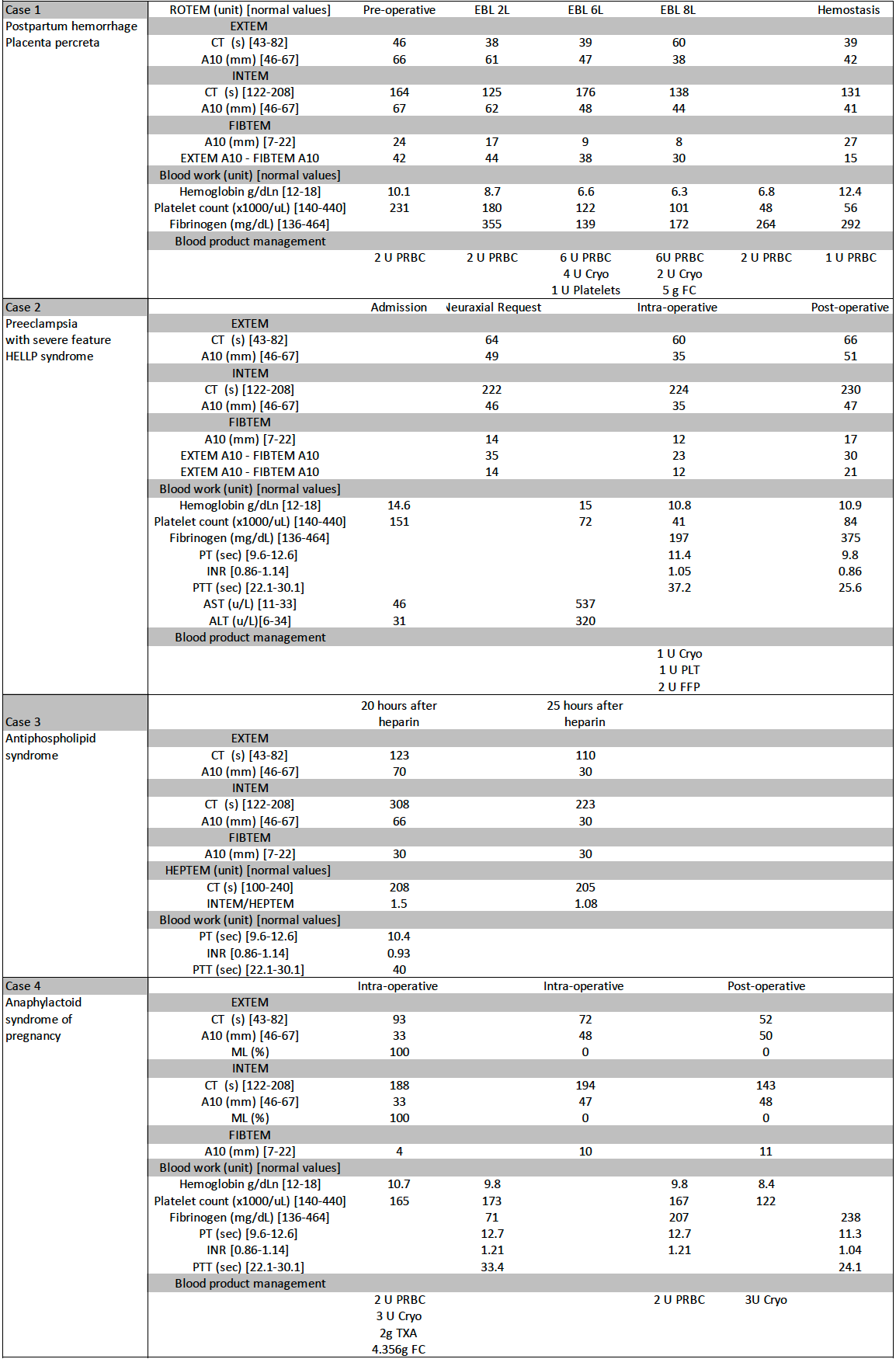
The use of point of care viscoelastic testing (POCVT) to guide hemorrhage management, decision making, and diagnosis is just starting to be explored. We present a case series exemplifying the use of the Rotational thromboelastometry (ROTEM) to guide blood product management during a postpartum hemorrhage, determine the safety of neuraxial anesthesia, tease out the effects of unfractionated heparin in a patient with abnormal baseline prothrombin time, and aid early detection of a coagulopathy when concerned for an anaphylactoid syndrome of pregnancy. We argue that POCVT monitoring can help anesthesiologists with more than just blood product management on the obstetrical floors.
Our articles most useful
Beth Turner, Charlotte Garrett and Anja Wittkowski
Published : February 13, 2018
Women's Health Research
Yinjia Guo, Min Zhao, Victoria Rutten, Yifei Gao, Arier Lee, Qi Chen
Published : November 22, 2017
Women's Health Research
Jessi Hanson-DeFusco*
Published : December 07, 2023
Women's Health Research
Dana R. Riedy, Sarah M. Ghose, Sahar M. Sabet, Morgan P. Reid, Claire M. Williams, Ashley MacPherson and Natalie D. Dautovich
Published : October 11, 2023
Women's Health Research
Peggy B. Smith MA*, Reginald Hatter, Jasmine King, Anne Van Horn and Sophie McCollum
Published : November 16, 2023
Women's Health Research
Shanette M. Harris
Published : August 22, 2022
Women's Health Research