The purpose of this study was to determine if there is a pattern to parents’ anger responses to emergency admission of their critically ill child to pediatric intensive care unit (PICU). Emergency admission of a child to PICU is stressful to both parents and the ill child. In dealing with their stress and frustration, some parents express their feelings through hostile behaviors towards their loved ones or towards health care providers. Knowledge of parental stress-induced anger levels will enable the PICU nurse to develop individualized assessment and intervention for parents not only upon admission, but also throughout their child’s stay in PICU.
An evaluative survey design was used with a group of 96 parents (68 mothers, 28 fathers) whose children were admitted to PICU on an emergency basis because of sudden illness or trauma. Parent-child dyad was used, but only parents’ anger responses were measured using the Zuckerman’s Multiple Affect Adjective Check List. Parents answered the same questionnaire every day for a maximum of five days and were asked to record their feelings on these particular days. Demographic data and types of procedures performed on the child were recorded daily.
Results indicated that parents’ anger level on the first day was at the 90th percentile levels as compared to normative sample of normal adults. On days 2, 3, and 4 parental anger responses dropped to 81, 86 and 79 percentile levels respectively, with no significant differences between days 2, 3, and 4. The major implication was that there is a pattern to parents’ anger responses. PICU nurses can be understanding of parental hostile behaviors and not be offended by it or take it personally. Parental behaviors of stress and their manifestations are contagious. It transmits from parent to the sick child. Helping parents deal with their feelings of anger will positively affect the recovery of their sick child.
*Corresponding Author:
Loucine M. Huckabay, Ph.D., PNP, RN, FAAN
Professor of Global Health and Nursing, Department of Health Science and School of Nursing, California State University, Long Beach, 1250 Bellflower Blvd., Long Beach CA, 90840 USA, Tel: (310) 413-1252; E-mail: Lucy.huckabay@csulb.edu
ABSTRACT
The purpose of this study was to determine if there is a pattern to parents’ anger responses to emergency admission of their critically ill child to pediatric intensive care unit (PICU). Emergency admission of a child to PICU is stressful to both parents and the ill child. In dealing with their stress and frustration, some parents express their feelings through hostile behaviors towards their loved ones or towards health care providers. Knowledge of parental stress-induced anger levels will enable the PICU nurse to develop individualized assessment and intervention for parents not only upon admission, but also throughout their child’s stay in PICU.
An evaluative survey design was used with a group of 96 parents (68 mothers, 28 fathers) whose children were admitted to PICU on an emergency basis because of sudden illness or trauma. Parent-child dyad was used, but only parents’ anger responses were measured using the Zuckerman’s Multiple Affect Adjective Check List. Parents answered the same questionnaire every day for a maximum of five days and were asked to record their feelings on these particular days. Demographic data and types of procedures performed on the child were recorded daily.
Results indicated that parents’ anger level on the first day was at the 90th percentile levels as compared to normative sample of normal adults. On days 2, 3, and 4 parental anger responses dropped to 81, 86 and 79 percentile levels respectively, with no significant differences between days 2, 3, and 4. The major implication was that there is a pattern to parents’ anger responses. PICU nurses can be understanding of parental hostile behaviors and not be offended by it or take it personally. Parental behaviors of stress and their manifestations are contagious. It transmits from parent to the sick child. Helping parents deal with their feelings of anger will positively affect the recovery of their sick child.
Key Words: Parental Anger, stress, PICU, emergency hospitalization.
INTRODUCTION
Emergency admission of a child to pediatric intensive care unit (PICU) is the most stress producing situation to apparent and the child [1-4]. Feelings of depression, anger, anxiety and post-traumatic stress syndrome have been found in parents of children admitted to a PICU both during as well as post PICU hospitalization [5]. However, none of these studies have looked at parental behavioral manifestations of stress in terms of anxiety, depression or anger on a daily basis to determine if there is a pattern to these behaviors. This study’s contribution to nursing and medical science is the determination of whether there is a pattern to the parental anger responses to their child’s unexpected emergency hospitalization to the PICU. Knowledge of parental anger responses in these situations, will enable the nursing and medical staff to intervene appropriately and help the parents deal with their anger response. In this study, the children who were admitted to the PICU were in perfect health may be half an hour ago or a couple of hours ago. But, due to an unexpected emergency such as a near drowning accident, or a car accident, or some other trauma, these children are rushed to the emergency room or to the PICU for a life-saving treatment. Parents are put into situations of making life and death decisions about the course of treatment to their children. Concern for the long-term consequences of this trauma such as mental or physical impairment, levels of pain and the very survival of their child are major sources of stress for parents of children who are admitted on an emergency basis [6, 7]. In dealing with their stress and frustration, some parents express their feelings through hostile behaviors towards their loved ones or towards health care providers. When sick children sense their parents’ anguish, they in turn become more stressed, depleting themselves of the energy they need for recovery [1, 2, 7].
Numerous studies have classified the causes of these stressors into three categories: (1) Personal-family stressors, (2) Situational stressors and (3) Environmental stressors. (1) Personal-family stressors are those that threaten parental roles, feelings of helplessness, other life stressors, parental age, educational level and personality factors such as propensity for anger or anxiety [1, 2, 8, 9].
(2) Situational stressors are those that deal with the child’s medical condition, diagnosis, acuity, amount of pain child is experiencing, outcome of the illness, fear of the unknown and the whole event of emergency admission of the child to PICU [1-3].
(3) Environmental stressors are those causes that are found in the physical environment of the PICU, such as, the sights and sounds of the emergency machinery and equipment, and those that are attached to the child, the tense environment of PICU that is often charged with urgency, and parent’s perception of the competency level of their child’s primary nurse [3, 7].
Parental Anger Feelings in PICU
Review of the literature revealed very few studies dealing with anger. Most PICU studies deal with the stress and anxiety levels and parental coping behaviors [1, 7]. It is not the PICU admission alone that has negative effect on the family, rather, the additive effect of how sick the child is on admission, the timing of the hospitalization, and the length of stay in the hospital were found to have negative consequences for the family [4].
Uncertainty over child’s outcome and family relationships that were found to be adversely affecting family’s coping and child management behaviors [10]. Additionally, if the doctors informed the parents that their child’s condition is incurable, or the child’s illness is irreversible, parents were found to reject, deny and exhibit hostile behaviors towards the doctors and medical staff. Parents also perceived that their child is being neglected [11].
Other variables that interfered with parental coping behaviors when their child was in PICU were the age and gender of the parent. For example, the study by LaMontagne et al [12] found out that older, more self-directed and less anxious parents were more likely to use coping strategies aimed at problem-solving and were more involved in caring for their sick child, than those who used more emotion-focused coping strategies.
With respect t to parental gender differences in response to their child’s PICU admission, the findings are conflicting. Women or mothers were found to exhibit more anger/hostility and despair than fathers when their child dies [13]. In another study, [14] women were found to express anger and sadness more often than men. Anger responses were twice more prevalent than sadness in women. Women also experienced distress 30% more than men. Men were found to keep their emotions to themselves, inhibit than women, whereas women expressed their feelings more freely. Theoretical perspective on male and female experience of anger implicates socialization patterns. That is, anger is perceived to be more acceptable for men and they inhibit or suppress better than women. It is not uncommon for women to express anger inappropriately [15]. Dutton et al [16] study found men’s anger-anxiety scores to be significantly higher than women’s in response to family conflict simulated situations, Conflicting findings were also found by Kopper & Epperson [17] study regarding whether anger expression is gender specific and as a result of socialization process. Their study did not find significant sex differences in anger expression or the tendency to suppress anger. Harris [18] found that different things provoke anger in males and females. Males consider physical hurt and women verbal insult to be more anger provoking. Thomas [19] found that men and women did not differ in their expression of anger. For both males and females, the correlates of anger symptoms were low educational levels, low optimism, poor health habits and external locus of control. Thomas also found that women who experienced more anger symptomatically were not suppressors of their anger, but directed it outward, taking it out on others and blaming others.
Parents, like other individuals who are under tremendous stress react to the situation by feeling extreme anxiety, anger and depression. In a previous study, Huckabay and Kessler [20] found that on the first day of an emergency admission of a child, parents’ anxiety level had reached 98 percentile level; This was two points short of being in a state of panic. According to Barris [21], extreme anxiety leads to anger. Parental anger can be directed either at themselves for not having protected their child from trauma, or it can be displaced anger aimed at others such as spouse, other kids, or health care personnel who may be perceived by a parent as not doing enough or not doing fast enough in caring for their sick child.
Several authors cite a need to conduct intervention studies on parents of children admitted to PICU [1, 7, 12, 22]. However, before such studies are undertaken, especially in areas of parental anger responses to emergency admissions of their child, it should be determined if there is a pattern to parental anger behaviors, so that PICU nurses can intervene more appropriately [2]. Therefore, the purpose of this study was to determine if there is a pattern to parent’s feelings of anger or when their child is admitted to the PICU on an emergency basis.
Theoretical Framework: Anger, Manifestations and Consequences
Anger is defined as an emotional syndrome consisting of set responses when human beings experience when they do not get what they think they should or must get or entitled to get, or when they are confronted with the realization that they cannot control others [21, 23]. Anger occurs in a social context or transitory situation. According to Roberts [24] anger is aimed at the correction of some perceived wrong. The perceived causes of anger are of two types: [1] Inhibited or Internalized anger. It refers to perceived threats involving blocked goals. E.g., Failure of an individual living up to parents’ expectations, disappointment, blow to self-concept, illness perceived as life threatening, physical dependence or altered social integrity, agents of harm [activator located in an authoritative position, family or self [24].
(2) Anger that is expressed directly or externalized refers to perceived threat involving obstructed goals, such as role changes or financial dependence. Agent of harm is located in the environment or the health care personnel.
Anger manifests itself at three levels: Physiological, Psychological and Socio-cultural
1. Physiological Level deals with the activation of the sympathetic nervous system [SNS] which increases adrenaline leading to increased heart rate, increased blood pressure, increased muscle tension, rapid and shallow breathing, sweating, . The arousal is the SNS leads to increased likelihood of aggressive verbal and/or physical behaviors, feelings of potency which makes the person want to confront the person against whom his anger is directed to. Anger results in the diminishing of problem-solving parental skills and interpersonal relationships skills. The person becomes very argumentative, verbally abusive and exhibits demanding behaviors [21, 24].
2. At the psychological level, anger is directed at the correction of some perceived wrong. When a person’s needs are not met, frustration and anger occur. Extreme form of anger becomes hate. According to Roberts [24], there are five types of hate: (a) Incipient hate is the type of anger that drives the person towards reprisal against the activator of the frustration. It is easiest to intervene before it escalates to a more vicious emotion [24]. (b) Inward hate is the condition when a person’s anger is directed towards oneself to avoid potential reprisals. Inward repressed anger often leads to other disorders and anxieties.
3. Explosive anger leads to explosive outbursts of behaviors without a warning effecting everyone on its path.
4. Deflective or displaced hate occurs when a person’s strong negative feeling is projected on another person or object without hurting the original activator or the perpetrator.
5. Constructive hate is the situation where the person is able to channel his/her anger more appropriately [24].
Often times, you see parents react angrily toward a nursing and or a medical staff for some minor thing that they perceive their sick child is not getting, If the original activator of parent’s anger is either themselves, as in near drowning incident due to parental neglect] or some other powerful person, then parents can displace their anger toward others for some minor perceived injustice or lack of entitled care to their child. One way of knowing if anger is displaced is by assessing its “proportionality”. When a person’s anger response is disproportionate to the activating event, that suggests that anger is being displaced [24].
6. Sociocultural level of anger refers to that anger that serves to uphold the accepted norms or standards of conduct [24].
Stress and Anger
Stress is an inevitable part of life. Appropriate levels of stress improve performance. Too low or too high levels of stress interfere with performance. Where does stress come from and why do individuals get angry? According to Barris [21], stress occurs when individuals wrongly believe that certain things external to them create their stress. Such as personal illnesses or illnesses in the family, financial problems, work -related problems or relationship related problems at home. As with anger and stress, things external to the individual carry no meaning other than the meaning the person chooses to give them. Some of these meanings or beliefs can result in destructive levels of stress, while others may be more helpful in reducing stress. Barris also points out when individuals assign meaning to events that produce high levels of stress, it predisposes them to become more vulnerable to responding more angrily to various activators in their life. In other words, under stress, the threshold of the potential to getting angry is lowered, thus anger can be ignited at the slightest activator of stress. Under normal circumstances, the same person would have managed the activator without being angry or stressed.
Relationship between Physiology of Anger and Intervention Strategies
Understanding the physiology of anger helps the management of anger. When a person becomes angry, the sympathetic nervous system (adrenaline) gets activated causing rapid heart rate, high blood pressure, muscle tension and sweating. When the person becomes aware of these changes in the signs and symptoms of anger, he/she should give oneself a “time out” from the activator. With the passage of time, other chemicals will breakdown the adrenaline in one’s system and the parasympathetic nervous system (PSNS) will intervene to help calm down the person. The process may take some time depending upon the person. There are certain things the angry person can do while waiting for the PSNS to intervene. For example, remove oneself from the presence of the activator, or do relaxation exercises if the activator remains in the situation. It is, therefore, important to remember that as parents recognize the early signs of anger , they can use tools for managing their anger that are physical, behavioral, cognitive, or emotional, by taking timeout, and doing controlled breathing and relaxation exercises, and by identifying and disputing anger producing beliefs [21]. In the PICU situation, if a nurse notices a parent being angry at self, or roughly pushing patient’s room furniture around or giving orders to the nursing or medical staff, the nurse acknowledge that they are in a stressful situation, and suggest if they (the parents) would like to take a coffee break, while she/he is taking care of their child.
Adverse Consequences of Anger
Anger-related activators are frequent problems that we encounter in our lives that we need to learn to solve them. According to Barris [21], anger has the same limiting effect on problem solving ability of the person as does the blinders on the horse’s eyes. It narrows a person’ s field of view so all a person sees are simplistic solutions that often are associated with some form of aggressive behaviors or attempt at controlling others. Barris [21] state that by converting anger into irritation, it peels off the blinders and the person can then see the whole range of possible solutions to that problem without being violent or controlling. For example, if the parent is angry about the high noise level in their child’s room and the constant loud speaker paging physicians, the nursing or medical staff can acknowledge that it is irritating or annoying but necessary, and offer if they can provide the parent an earplug, as they do in the airplanes.
Anger can kill a person. Research by Barris [21] has shown that a person with uncontrolled anger is at a greater risk of heart disease, high blood pressure, headaches strokes and stomach related problems. Also, persons with higher levels of anger at age 25 are 4-7 times more likely to be dead at age 50 than those persons with lower levels of anger. Anger also destroys important relationships; society punishes angry people who behave aggressively.
Operational Definitions
Anger/Hostility: It refers to the unfavorable affective reactions experienced buy parents, exhibited by such behaviors as annoyance, complaints, being cross and critical, disagreeable, incensed, irritated, furious, mad mean, enraged, as measured by Zuckerman’s Multiple Affect Adjective Check List (MAACL). It is aimed at correcting some perceived wrong.
Patterns of Parental Responses to Stress: It refers to trends in variations of parents’ reactions and behaviors towards the changing conditions and events occurring in their critically ill child while in PICU.
Child: A human being between the ages of birth to 18 years of age,
Emergency Admission: This is an unplanned admission of a child to the PICU because of a sudden life-threatening medical condition.
Critical: It refers to the classification /acuity of a patient’s medical condition that is life-threatening and requires admission to the PICU on an emergency basis for immediate medical and nursing intervention.
Methodology
Design: An evaluative survey design was used. Parent’s anger levels were measured daily for the duration of their child’s stay in the PICU for a maximum of 5 days. The PICU was 2/4 days.
Participants: The sample consisted of 96 parents [68 (70.8%) mothers and 28 (29.2%)] fathers of 765 children admitted with a sudden life-threatening illness to the PICU from the emergency department or another hospital. Children from birth to 18 years pf age were admitted to the study if they had no history of present or chronic illnesses, no history of previous hospitalization or child abuse. Their diagnosis included trauma, car accident, near drowning, aspiration, poisoning, Reye’s Syndrome, meningococcemia and encephalopathy. Parent selection criteria included they had to speak English, not be a health care worker or professional. The child had to live with the parents.
Setting: The study setting was a 22-bed PICU where parents could visit their child 24 hours a day. Because all the patients were admitted to the PICU on an emergency basis, they were all considered critical on admission, so the patient’s acuity was not measured. Each child had a cardio scope and intravenous lines, but only 15 (19.7&) required ventilator support.
Instruments: The anger component of MAACL was used. It consisted of ----adjectives and measured parents’ daily anger levels. Scoring of the survey was done by counting the number of items checked each day, The total score could range from 0 to----. Zuckerman and Lubin (25) established the tool’s concurrent validity by correlating it with Taylor’s Manifest Anxiety Scale (r= .55; p<.05) and with Cattell’s IPAT Anxiety Scale (r = .55, p<.05). They determined the tool’s reliability using the split-half method on college students and psychiatric patients. The reliability coefficients were 0.79, p<.01, and 0.74, p<.01, respectively, indicating the tool’s internal consistency.
The child’s medical chart was reviewed to identify procedure performed each day using a check list of medical procedures such as intubation, extubation, insertion of lines, tests, nursing procedures, and change in patient’s condition. This information was used to determine if the number of procedures correlated with parents’ daily anger levels. Content validity was established through the literature [3, 4, 6, 19].
Interscorer reliability between the researcher and the research assistant yielded 97% agreement. Demographic data, including the child’s age, sex, birth order, and diagnosis and parents’ ages, religion, and education level, were obtained to determine whether these factors were related to parents’ anger levels.
Procedure: The study was approved by the Institutional Review Board of both the university and the hospital, and parents gave written consent. While the parents were waiting in the waiting room or at their child’s bedside, they were given the questionnaire to complete. They were instructed to check only those items that described their feelings today—right now. The parents were given the same questionnaire again the next day and were instructed to check those items that expressed their feeling that day. Testing was repeated once a day for the duration of their child’s stay in the PICU or a maximum of 5 days.
Data Analysis: The raw scores were converted to t-scores based on the test manual’s instructions (25). Anger levels were compared using the matched t-test to determine if significant differences existed between the anger levels on different days, and to determine if anger levels had a trend. Because there were only two subjects still left in the PICU on day five, data from day five was not included in the data analysis. Pearson’s Product Moment Correlations (r) and Chi Square tests were done, as appropriate, to determine if the demographic data and the number of procedures and treatment performed on each day were related to parents’ anger levels on each of the days of the child’s hospitalization in PICU.
To determine if significant differences existed in the number of procedures and tests performed on each of the days, matched t-test were performed. Because of the numerous variables, Bonferroni’s correction for multiple tests was conducted. A p-value of .005 was determined to be the level of statistical significance.
RESULTS
Results are presented in the order of the major research questions followed by the significant relationships between the demographic data and the anger/hostility behaviors.
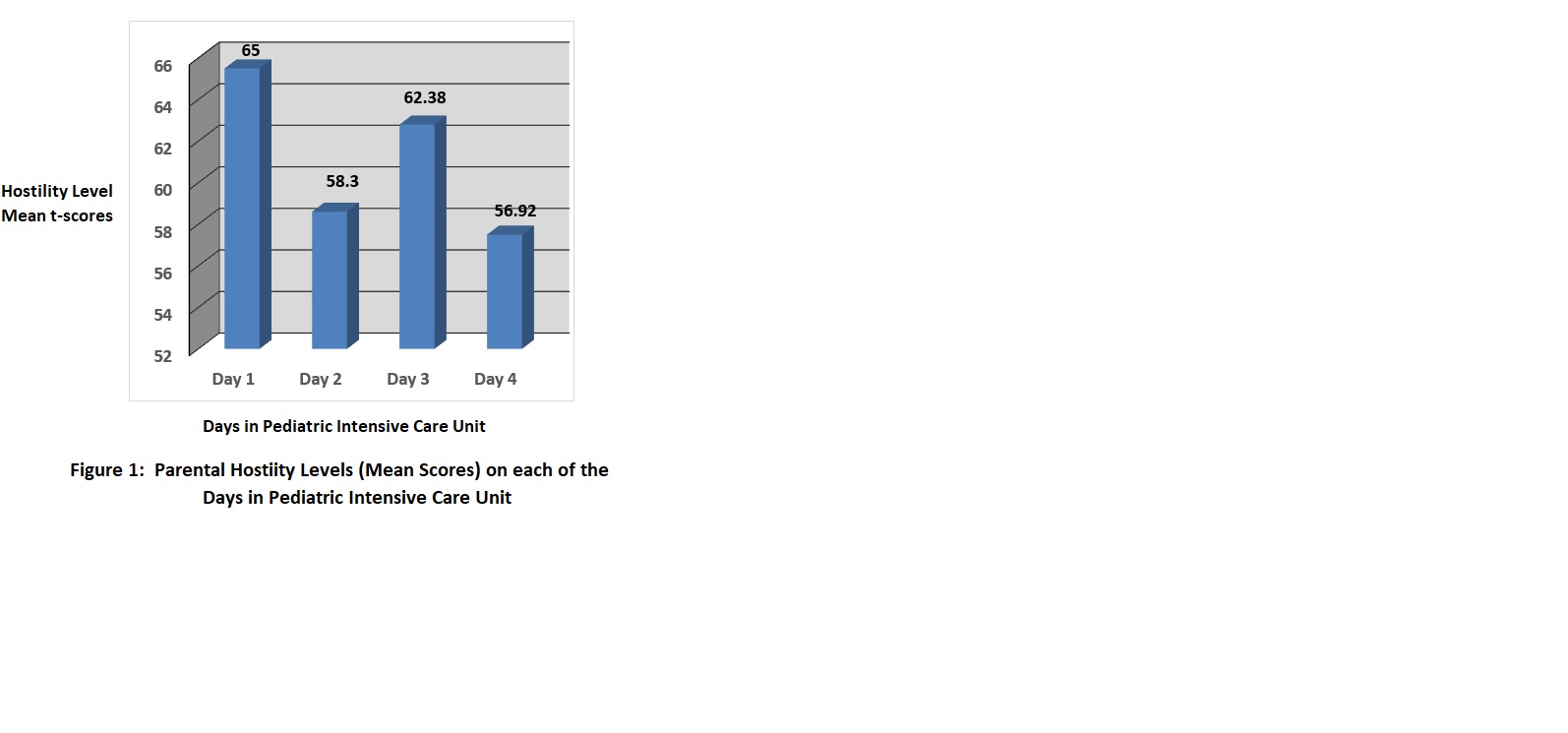
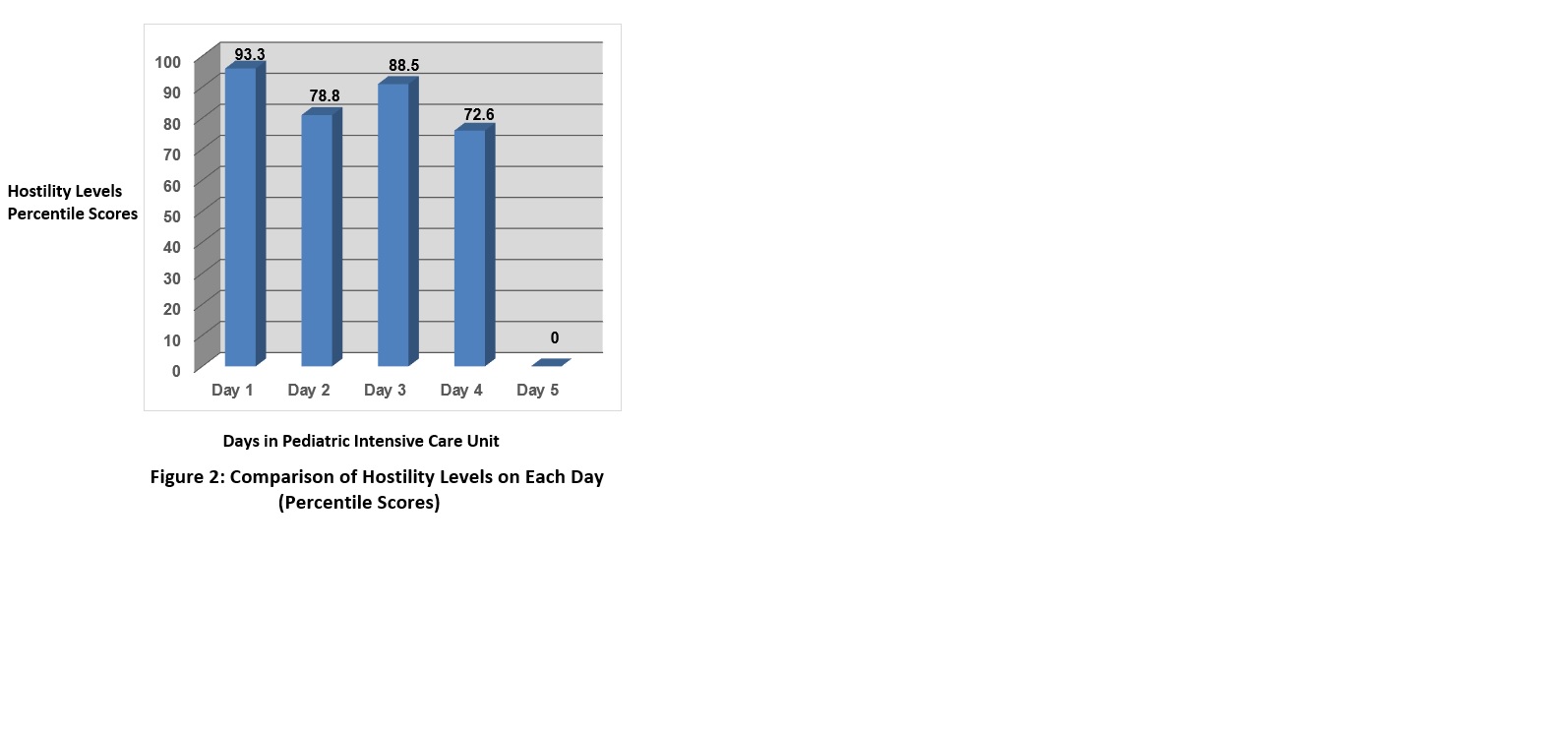
The first research question asked, what is the anger/hostility levels of the parents whose children are admitted to PICU on an emergency basis? In order to compare parents’ anger levels to the norms (normal people) that were provided by the tool’s manual [25], the parental raw scores on anger had to be converted to t-scores and then compared to the established norms. Table 1 and figure 1 show that the parental anger scores were significantly higher (p<.0001) than the norm. T he average length of stay (LOS) for the group was 2.36 days. On day 1 through 4, the mean scores were 65, 58.30, 62.38, & 56.92 respectively. When these mean T-scores were converted to percentile scores, on the first day parental anger score was at 93.3%, on days 2, 3, and 4, the percentile scores were 78.8%, 88, 5%, and 72.6% respectively. Results are presented in Figure 2. At the 98 to 100 percentile level, rage or hate would be expected [24, 25].
The second research question asked, is there a pattern to the parental anger behaviors when their child is admitted to the PICU on an emergency basis? Comparison of means between each of the days on anger behavior were conducted using the matched t-tests. Results presented in Table 3 show that there was a significant difference (t = 3.90, p<.0001) between days 1 and 2. There were no significant differences between the other days. However, going back to percentile scores presented in figure 2, the pattern observed is that parents are significantly angrier on each of the days when compared to the norm, with first day reaching at the 93.3% levels and the third day at the 88.5% level. On Days 2 and 4, the anger levels were lower, but still significantly higher than the norms. The standard deviations of this study are comparable to the norm. In this study, the results are reported in percentiles compared with the norm, with 50 percentile representing the mean and the median [25, 26].
Additional Findings
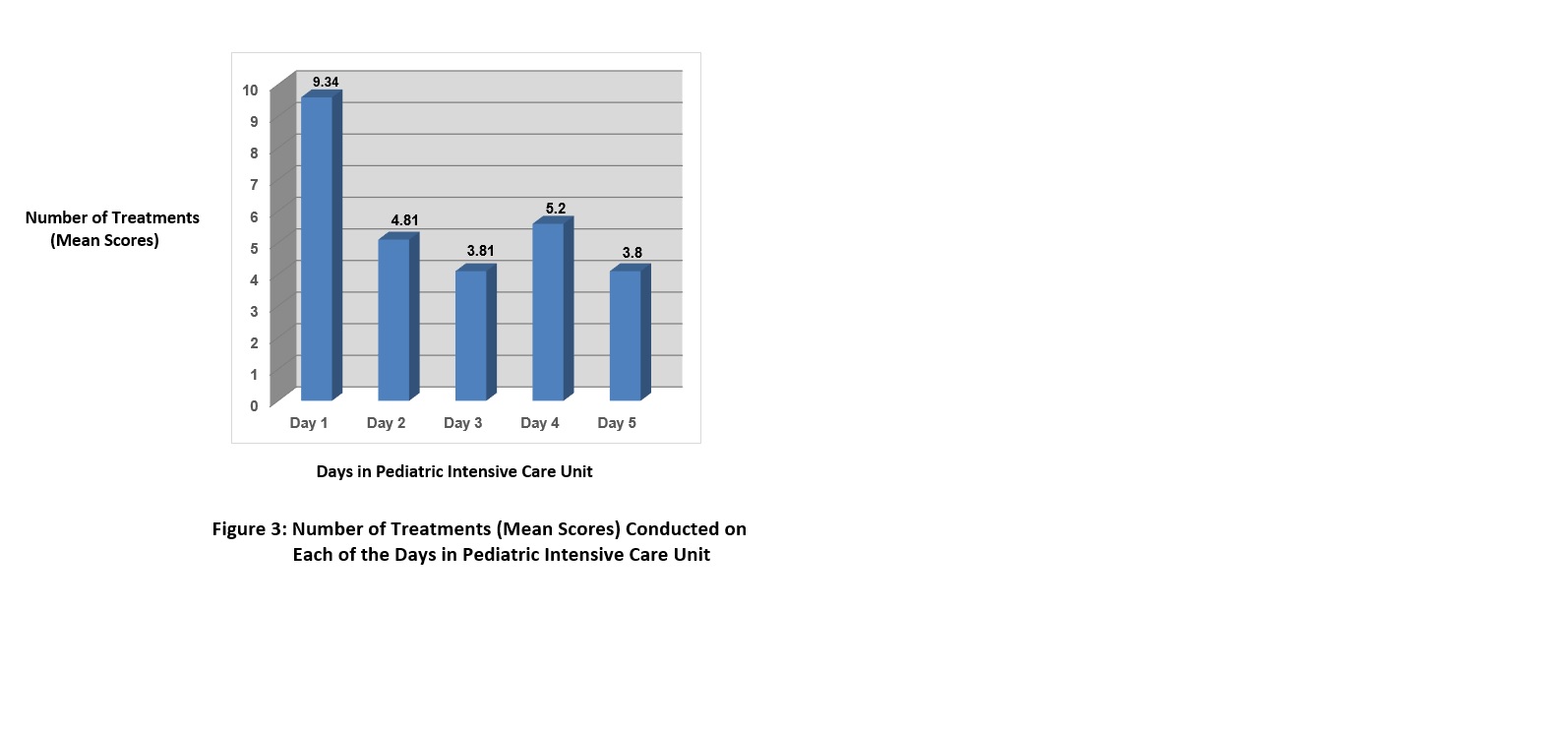
When all the variables were related to one another using the Pearson Product Moment Correlation, findings presented in Table 6 show that overall, the anger scores are significantly and positively correlated to one another. Also the total number of procedures performed on the child was also positively and significantly related to hostility behaviors. The correlations ranged from .38 to .48, all significant at the p< .005 levels. The mean number of procedures performed on days 1 through 5 were 9.34, 4.81, 3.81, 5.2 & 3.8 respectively. Results are presented in Figure 3.
The child’s age, birth order, parental age, educational level and LOS of the child were not found to be related to anger behaviors. Lastly, when mother’s anger behaviors were compared to the father’s using the t-test for independent means, maternal anger behaviors were higher than the fathers on each of the days, however, none reached significant levels. Results are presented in Table 4.
DISCUSSION
Findings on the major research question indicate that there is a pattern to parental anger response to the emergency admission of their critically ill child throughout their child’s stay in the PICU. Very High anger level was observed on the first day, followed by significant reduction in day-2, resurgent fluctuation on day-3 and stabilization on day-4.
On the first day, parents’ very high anger level was consistent with Barris, [21] Ellis [23] and Roberts’ [24] theories on the positive relationship between stress and anger. When a person or a parent assigns meanings to events that result in high levels of stress, that parent or the individual is making himself/herself more vulnerable to responding angrily to the various activators in his/her life. Under stress, a person’s threshold to respond angrily to a given activator is lowered. In a previous study, Huckabay & Kessler [20] found that parents whose children were admitted to PICU on an emergency basis experienced near panic level (98th percentile) of stress and anxiety. The types of meanings parents assign to the emergency admission of their very critically ill child may be -- the possible loss of their child’s life or health, and potential of their parenting role, which they hold essential to their psychological integrity and parenting responsibilities [7, 22]. Additionally, the three categories of stressors as identified by Miles and associates [7] – the personal-family stressors, environmental and situational stressors—can also serve as activators that increase the parental stress levels and lowers their anger threshold.
Another possible reason that could explain the very high anger level on the first day may be due to the parental feelings of powerlessness in their inability to nurture and protect their child from feelings of pain at the critical time. Parents’ level of participation in their child’s care was also very limited on the first day, because of constant presence of medical and nursing personnel in the room, treatments and multiple tests. It was not uncommon to see parents being critical at the medical and nursing personnel if they perceived that their child was unduly experiencing pain, or that the medical and nursing personnel did not respond fast enough to their child’s requests or self-perceived needs. Feeling angry at the medical and nursing personnel may give a parent the feeling of power in the face of powerlessness. This may be a form of displaced anger and is consistent with Baris [21] and Robert’s [24] conceptualization of displaced anger, where the strong negative feelings of anger are projected on to another person or object, without hurting the original activator of anger, which may be themselves, or another powerful person .
Another possible explanation for their anger that takes place in the form of a displaced anger may be that if the cause of their child’s sudden critical illness was due to some form of a preventable parental neglect, as in a near-drowning accident, or an accidental ingestion of a toxic substance by the child, or a trauma as in a car accident or fall, the parent may feel angry at self (internalized repressed anger) or project it onto others in the form of displaced anger.
To summarize, the very high parental feelings of anger on the first day of their child’s sudden hospitalization to PICU may be due to the high levels of stress parents experience which lower their threshold for feeling anger, or the meaning they place on the activator which increases their stress, makes them feel powerless. These feelings of anger are then expressed either internalized towards the self, especially if the cause of the child’s sudden illness was due to a preventable parental neglect, or anger is displaced or projected on to another person or object, if the activator is either self or another powerful person.
Days Two through Four
On day-2, parental anger levels dropped significantly, and there were no significant differences between days- 2, 3, and 4. The percentile anger scores were 78.8, 88.5, 72.6 respectively. The resurgence of anger on Day3 and subsequent drop to 72.6% level may be due to the fluidity of feelings of anger with the trend toward possible stabilization.
This explanation is consistent with Barris’ [21] and Ellis [23] conceptualization of the relationship between physiology of anger and intervention strategies. When a person gets angry, the sympathetic nervous system (SNS) the adrenaline level is activated with the resulting in physiological signs and symptoms, as in the case on the first day of their child’s emergency hospitalization in PICU. As the child survives the first day and as the number of procedures the child needed on subsequent days decreased significantly after the first day, the parental stressors decrease. This is like taking “time out” from the activator. With passage of time, other chemicals will breakdown the adrenaline in one’s system and the parasympathetic nervous system (PNS) will intervene to help calm down the person (parent). This process may take some time depending on the person. Barris [21] states that there are things a person can do while waiting for the PNS to intervene. Removing oneself from the presence of the specific activator or by using relaxation techniques, one can calm oneself down while still remaining with the activator. In light of this conceptual framework, as the stressors were decreasing and as the nursing and medical staff intervening with the child and possibly also helping the parents cope with situation through explanation, proper communication to relieve parental anxiety, these could possibly were serving as “time outs” and enabling parents to relax, not be as anxious as day-1, while still remaining with their ill child. Additionally, if therapeutic communication with the parents enabled the parents to identify and dispute their anger producing beliefs, then it would possibly explain the reduction of anger on subsequent days.
The differences the average number of days between day 1 and 4 fell short of significance (p< .10) level, even though there were 20.7 percentile point differences between the two days .This may be due to the smallness of the sample size on day 4. There were only 12 subjects left in the PICU on the fourth day. The average number of days in the ICU was 2.36 days. That is on the third day, most of the children were well enough to be transferred to the pediatric floor.
The resurgence of anger responses to 88.5%level on the third day may be due to the possibility that for some parents, it is difficult to get rid of their anger, especially if it serves them in getting what they want and in making them feel that they have control. Also it may be that physiologically, their PNS has not yet intervened to calm them down. Although these explanations are consistent with Barris’ [21] physiological theory of anger, it awaits further testing, as this study did not measure parental physiological responses to anger.
Overall, parental anger scores were reduced and somewhat stabilized at the 72.6% level on the fourth day. They are still moderately high [25]. This may have been due to unresolved situational stressors, such as uncertainty about the long-term consequences of their child’s illness, financial concerns, and worries about other children left at home. Additionally, those parental anger producing beliefs that have not been completely disputed may still continue to fester for a while producing the moderate amounts of anger responses in parents [2, 3].
Additional Findings:
The only significant additional finding was the positive relationship between anger responses between the different days. This points of to the construct validity of the zuckerman & lubin’s [25] anger/hostility tool.
Implications of the Study
The implications to nursing practice are based on the findings of the study and the literature review.
These are means by which the critical care nurses can help parents whose children are admitted to PICU on an emergency basis.
Be Aware of the high anger level on Day-1.
When PICU nurses are aware of the daily patter pf anger and hostility behaviors, they can intervene quickly and appropriately. Assessment of both overt and covert signs of parental anger gives nurses additional knowledge to anticipate parents’ anger levels and subsequent behaviors to intervene.
Because of the very high level of anger on the first day, nurses should assess parents for:
• Extreme criticism of nursing and medical staff.
• Near enrage look
• Disproportionate expression of volatile voice tone.
• Extreme muscle tension such as clenched fist, clenched jaw, excessive muscle movements.
• Complaints of headaches, stomach ache.
On admission day. When parents’ anger levels are very high, The PICU nurses’ primary responsibility is to provide support by allowing parents to talk about how they are feeling and by answering questions about child’s condition and care as fully as possible.
Know the causes of stressors and their relationship to anger/hostility.
In this study, on the admission day, every time a nurse or a physician entered the room or performed a procedure, the parents wanted to know how their child was doing, and if everything possible being done on their child. The overall picture of the child’s condition is very important to parents. Nurses can help parents see progress and explain to them very simply the purpose of each treatment. Data from this study showed that the number of procedures performed on the child was positively and significantly related to hostility /anger behaviors of the parents.
Miles and Associates [7] identified three sources of parental extreme stressors in the PICU settings: the personal-family, situational and environmental stressors. Barris [21] and Ellis [23] pointed out that when parents are very stressed, their threshold to deal with anger-related activators are lowered leading parents to being angry and hostile to seemingly minor situations. When PICU nurses understand the relationship between stress and anger, they can anticipate these feelings, communicate therapeutically with parents and not take parental anger as being directed to them.
Be aware of displaced anger
As the literature [21, 24] pointed out, one of the psychological manifestations of anger is displaced anger, where parents’ project their hostile/anger behaviors into other objects, situations, or persons. This is true when the original activator (cause) of the anger is too powerful, or they are afraid of reprisal, or the activator may be absent, or it can be themselves. In this situation, if the PICU nurses can recognize the signs and symptoms of displaced anger, they will not take the potential hostile behaviors personally. Signs to watch are:
• Disproportionality of parental anger response to seemingly minor event.
• Parents hitting or roughly handling inanimate objects in the surrounding.
• Overt verbal accusations towards nursing and medical staff or to others.
• Extreme criticism of others for having caused their child to be ill. This may be directed toward God or some other supernatural situation or blame their luck or fortune or “bad eye”.
In these situations, if the PICU nurse can stay calm, and let the parents vent their feelings and acknowledge their feelings later, as parents calm down, the nurse can explain the treatments/procedures they are doing on the child and provide a listening ear to parents. It is important for PICU nurses to be aware that displaced anger does not necessarily mean that the nurse has done anything wrong.
Be Aware of Parental internalized Anger
Literature [21, 24] also tells us that parental anger can be internalized towards themselves and be repressed. Consequences of repressed anger can lead to other disorders. This condition can occur if the child’s condition occurred as a result of possible preventable cause. PICU nurses can watch for such behaviors as:
• Parental self-blame.
• Expression of negative feelings towards self.
• Covert self-punishing behaviors.
• Behaviors “to make up” possible neglect.
• Taking on to them undue blame.
Awareness of these behaviors by the PICU nurse, can allow her to communicate therapeutically to the parents by acknowledging their feelings, provide accurate information about child’s situation and be available to parents. If the PICU nurse observes some pathologically self-destructive behaviors in parents, she should refer them to psychological counseling.
Encourage Parents to Ask Questions
Encouraging parents to ask questions and express their feelings and concerns helps them to relieve some of their anxieties, stresses thus diffuse anxiety-related anger feelings. On Day-1, when stress and anger levels are very high, parents may not know what to ask. Nurses can explain in simple words, the purpose of the tests, and if their child is maintaining the status quo, and any changes in condition.
Empower Parents
One of the causes of parental anger when a child is admitted to PICU on an emergency basis may be the loss of control over the situations and possible loss of their parental nurturing roles [7, 21]. PICU nurses should be sensitive to any indications from parents who want to help in their child’s care, especially after the first day of admission, when their anger levels are lower. Participating in their child’s care enables parents to resume their parenting and nurturing role. When parents’ needs are met, they can become effective partners in their child’s health and recovery [26].
Identify Variations from the Pattern
By recognizing the anger and stressor patterns, nurses can identify parents who vary from it. If parents are apathetic or vary in other ways from the usual pattern, PICU nurses should closely assess parental responses. Especially with trauma emergency admissions, possible abuse may need to be investigated [20].
Allow Time and Provide Therapeutic Relaxation Techniques
Barris [21] and Ellis [23] point out that when people are angry their sympathetic nervous system and the adrenaline levels are on high alert and inaction. It takes time for the physiological responses to subside in order for parasympathetic nervous system to take place. One-way PICU nurses can help the parents during this waiting period is to help and teach parents how to do relaxation breathing exercises and imagery to calm them down. As anger levels are lowered, parents are more capable of doing child-care related problem-solving and decision making.
Provide Continuity on Transfer from the PICU to the General Pediatric Unit
On the third day of admission to the PICU, parental anger behaviors were elevated compared to the second and fourth day. Findings of this study showed that the average length of stay in PICU was 2.6 days, meaning that most children were transferred from the PICU to the general pediatric floor. Nurses might expect parents stress and anger levels to decrease significantly on the third day, but it did not. Therefore, nurses need to refocus on the parents before their child is transferred from the PICU to the floor by:
• Explaining to parents ahead of transfer the improved condition of their child.
• Stress the expert capabilities of pediatric nurses on the general floor in caring for their child.
• Orienting the parent to the pediatric floor and introducing them to the nurses prior to transfer.
• Reassuring the parents that their child will not need the PICU-related equipment on the general floor.
• Both PICU nurses and general pediatric floor nurses need to be aware of parental transfer anxiety (stress) both from PICU to the floor and again upon getting the patient to be discharged to home. In both cases, nurses need to prepare, teach, and reassure parents for these events. Also, provide parents with appropriate telephone numbers of doctors, or emergency department should they need to call for any questions.
Limitations of the study
The study sample is relatively small (N=96). Generalizations should be made with caution. Study findings should not be generalized to the relatives of adult critical care patients, nor to other PICU patients who are not admitted on an emergency basis. Since all patients in this study were admitted under extreme emergency conditions, their acuity levels were not differentiated which may have influenced parental anger levels.
Recommendations for Future Research
To replicate the study with a larger sample so that generalizations can be made with more confidence. To study the effect of different types of intervention strategies to help parents cope with these intense feelings of stress and anger and other negative emotions, such as depression, which are associated with emergency admission of a child to PICU.
Summary and Conclusion
This study found that parents’ anger/hostility levels were extremely high on the first day of their child’s emergency admission to PICU compared to the normative sample of adults. On second day, it was significantly reduced with some resurgence of anger behaviors on the third day, which may have been due to child’s transfer to the general pediatric floor. On the fourth day, anger behaviors were dropped the lowest at the 72.6% percentile levels indicating a trend toward stabilization. With this knowledge, PICU nurses can assess parents’ anger/hostility levels and adapt their therapeutic communication and teaching strategies accordingly.
REFERENCES
1. Alzawad, Z. Lewis, F. M., & Walker, A. (2022). Parents’ challenges beyond the pediatric intensive care unit: Fraying at the seams while balancing between two worlds, home and hospital. Children, 9, 267-276.
2. Alzawad, Z., Weiss, J M., Lee, J., Perkhounkova, Y., Hein, M., & McCarthy, A. M. (2024). Exploring factors affecting parental psychological vulnerability during their child’s PICU admission: A prospective pilot cohort study. Journal of Pediatric Health Care, 38(3), 323-336.
3. Debelic, I., Mikolcic, A., Tihomirovic, J., Baric, I., Lendic, D., Niksic, Z., Sencaj B., & Lovric, R. (2022). Stressful experiences of parents in the pediatric intensive care unit: Searching for the most intensive PICU stressors. International Journal of Environmental Research and Public Health, 19(18), 11450-11474.
4. Youngblut, J. M., & Lauzon, S. (1995). Family functioning following PICU hospitalization. Issues in Comprehensive Pediatric Nursing, 18(1), 11-25.
5. Logan, G. E., Sahrmann, J.M., Hongjie, Gu., & Hartman, M. E. (2020). Parental Mental health care after their child’s pediatric intensive care hospitalization. Pediatric Critical Care Medicine, 21 (11); 941 - 948.
6. Toly, V. B., Zauszniewski, J. A., Wang, M., Russell, K. N., Ross, K., & Musil, C. M. (2024). Efficacy of a resourcefulness intervention to enhance the physical and Mental health of parents caring for technology-dependent children at home: A Randomized controlled trial. Journal of Pediatric health Care, 38 93), 337-353.
7. Miles, M. S. et al (1989). A consortium study of parent stressors in the pediatric ICU. Maternal Child Nursing Journal, 18, 181-243.
8. Stremler, R., Haddad, S., Pullenayegum, E., Parshuram, C. (2017). Psychological outcomes in parents of critically ill hospitalized children. Journal of Pediatric Nursing, 34, 36-43.
9. Hagstrom, S. (2017). Family stress in pediatric critical care. Journal of Pediatric Nursing, Nursing Care, Children and Families, 32, 32-40.
10. Tomlinson, P. S., Kirschbaum, M., Harbaugh, B., & Andersen, K. H. (1996). The influence of illness severity and family resources on maternal uncertainty during critical pediatric hospitalization. American. Journal. of Critical Care, 5(2), 140-146.
11. Waller, D.A., Todres, I. D., Cassem, N. H., & Anderton, A. (1979). Coping with poor prognosis in the PICU. The Cassandra Prophecy. American Journal of Disabled Child, 133(11), 1121-1125.
12. La Montagne, L. Hepworth, J. T., Pawlak, R., & Chiafery, M. (1992) Parental coping and activities during pediatric critical care. American Journal of Critical Care, 1(2): 76-80.
13. Schwab, R. (1996). Gender differences in parental grief. Death Studies, 20(2), 103-113.
14. Mirowsky, J., & Ross, C. E. (1995). Sex differences in distress: Real or artifact? American Sociological Review, 60(3), 449-468.
15. Sharkin, B. S. (1993). Anger & gender: Theory, research and implications. Journal Of Counseling and Development, 71(4), 386-389.
16. Dutton, D. G., Webb, A. N., & Ryan, L. (1994). Gender differences in anger/anxiety reactions to witnessing dyadic family conflict. Canadian Journal of Behavioral Sciences, 26(3), 353-364.
17. Kopper, B. A., & Epperson, D. L. (1991). Women and Anger: Sex and Sex Role. Comparisons in the expression of anger. Psychology of Women Quarterly, 15(1), 7-14.
18. Harris, M. B. (1993). How provoking? What makes men and women angry? Aggressive Behaviors, 19(5), 199-211.
19. Harris, M. B. (1993). How provoking? What makes men and women angry? Aggressive Behaviors, 19(5), 199-211.
20. Huckabay, L. M. D., & Tilem-Resnick, D. (1999). A study of parental daily stress levels in PICU in an emergency admission. Dimensions of Critical Care Nursing, 18 (2): 36-42.
21. Barris, B. P. (1999). When Chicken Soup Isn’t Enough: Managing Your Anger in an Increasingly Angry World. Smiling Warthog Publishers.
22. Lazarus, R. S., & Launier, R. (1978). Stress-related transaction between person and environment. In L. A. Previn, & M. Lewis (Ed.), Perspectives in International Psychology. (pp 287—327). Plenum Press. New York.
23. Ellis, A. (1977). Anger: How to Live with and Without, A Citadel Press Book, Carol Publishing Group.
24. Roberts, R. L. (1986). Behavioral Concepts and the Critically Ill Patient. 2nd Ed. Appleton Century Crofts.
25. Zuckerman, M., & Lubin, B. (1985). Manual for the MAACL-R, The Multiple Affect Adjective Check List Revised, San Diego, Calif.: Edits Publishers.
26. Farrell, M. F. & Frost, C. (1992). The most important needs of critically ill children: Parents’ perceptions. Intensive and Critical Care Nursing, 8, 130-139.
27. Munro, R. H. et al, (1986). Statistical Methods for Health Care Research, J. B. Lippincott.
PEER REVIEW
Not commissioned. Externally peer reviewed.
TABLES
Table 1: Comparison of means between the anger levels of parents using the t-test for independent means on each of the days.
|
Days |
Means |
SD1 |
t-value |
p-value |
|
1 |
65.00 |
13.20 |
48.24 |
.0001 |
|
2 |
58.30 |
15.60 |
28.97 |
.0001 |
|
3 |
62.38 |
14.82 |
22.66 |
.0001 |
|
4 |
56.92 |
14.07 |
14.02 |
.0001 |
Table 2: The percentile score of hostility behaviors for each of the days in Pediatric Intensive Care Unit
|
Days |
Means |
Percentile |
|
1 |
65.00 |
93.3% |
|
2 |
58.30 |
78.8% |
|
3 |
62.38 |
88.5% |
|
4 |
56.92 |
72.6% |
Table 3: Comparison of means of parental anger behaviors between each of the days using the matched t-test.
|
Comparison of Days |
|
|
|
|
|
Day 1 |
66.27 |
13.16 |
3.90 |
.0001 |
|
Day 2 |
58.3 |
15.72 |
||
|
Day 1 |
66.04 |
12.21 |
1.22 |
.23 |
|
Day 3 |
61.54 |
14.33 |
||
|
Day 1 |
68.42 |
14.02 |
1.78 |
.10 |
|
Day 4 |
56.92 |
14.07 |
||
|
Day 2 |
60.71 |
12.99 |
-.39 |
.69 |
|
Day 3 |
61.54 |
14.33 |
||
|
Day 2 |
57.83 |
8.50 |
-.30 |
-.77 |
|
Day 4 |
56.92 |
14.07 |
||
|
Day 3 |
62.38 |
13.11 |
-.39 |
.70 |
|
Day 4 |
56.92 |
14.07 |
Table 4: Comparison of means between fathers and mothers for the total group on hostility measures on each of the days using t-test for independent means.
|
Variable |
Mothers Means (SD1) |
Fathers Means (SD1) |
t-value |
p-value |
|
Hot Tot |
62.79 (12.00) |
61.54 (12.54) |
.42 |
.65 |
|
Host 1 |
65.12 (12.73) |
64.71 (14.52) |
.14 |
.89 |
|
Host 2 |
59.03 (15.28) |
56.85 (16.48) |
.51 |
.61 |
|
Host 3 |
64.78 (15.56) |
58.45 (13.28) |
1.12 |
.27 |
|
Host 4 |
58.50 (15.57) |
53.75 (11.81) |
.53 |
.61 |
Table 5: Comparison of mean differences between each of the days and the numbers of procedures performed on the child in Pediatric Intensive Care Unit, using the match t-test.
|
Between Day Comparison |
N |
Mean Differences |
SD1 |
df |
t-value |
p-value |
|
1&2 |
68 |
5.5 |
5.3 |
66 |
8.41 |
.0001* |
|
1&3 |
32 |
6.2 |
5.3 |
30 |
6.67 |
.0001* |
|
1&4 |
15 |
3.5 |
4.9 |
13 |
2.78 |
.01 |
|
1&5 |
5 |
3.4 |
3.2 |
3 |
2.37 |
.08 |
|
2&3 |
32 |
1.6 |
2.7 |
29 |
3.36 |
.002 |
|
2&4 |
15 |
1.1 |
3.1 |
13 |
1.41 |
.18 |
|
2&5 |
5 |
3.0 |
1.6 |
3 |
4.24 |
.01 |
|
3&4 |
15 |
-0.3 |
1.7 |
3 |
0.75 |
.46 |
|
3&5 |
5 |
0.6 |
3.6 |
3 |
0.37 |
.73 |
|
4&5 |
5 |
1.2 |
1.8 |
3 |
1.50 |
.21 |
*Significant
Table 6: Correlation matrix for all the variables for the entire group using the Pearson Product Moment Correlation (r).
|
Variable |
Hot Tot |
Host 1 |
Host 2 |
Host 3 |
Host 4 |
|
Hot Tot |
1 |
78*** |
89*** |
78*** |
69** |
|
Host 1 |
1 |
41** |
11 |
26 |
|
|
Host 2 |
1 |
67**** |
66** |
||
|
Host 3 |
1 |
.52 |
|||
|
Host 4 |
1 |
||||
|
C Age |
.12 |
.12 |
.01 |
-.29 |
-.37 |
|
B Order |
.19 |
.12 |
.14 |
-.14 |
.21 |
|
M Age |
.18 |
.1 |
.14 |
-.19 |
-.17 |
|
F Age |
.14 |
.06 |
.08 |
-.11 |
-.19 |
|
#Proc Tot |
.31*** |
.31*** |
.48*** |
.32*** |
.24 |
|
Proc 1 |
.22 |
.23 |
.34** |
.08 |
.01 |
|
Proc 2 |
.40 |
.23 |
.49**** |
.44** |
.35 |
|
Proc 3 |
.34 |
.25 |
.37 |
.31 |
.22 |
|
Proc 4 |
.57 |
.47 |
.51 |
.28 |
.14 |
|
LOS |
-.05 |
.04 |
.05 |
.07 |
.48 |
|
Educ |
-.19 |
-.14 |
-.24 |
-.38 |
-.29 |
** = p<.01
*** = p<.001
**** =p<.0001
Host Tot = Total score on hostility behavior
Host 1= Hostility score on 1st day
Host 2= Hostility score on 2nd day
Host 3= Hostility score on 3rd day
Host 4= Hostility score on 4th day
#Proc Tot = Total number of Procedures
Proc 1= Number of procedures on Day 1
Proc 2 = Number of procedures on Day 2
Proc 3 = Number of procedures on Day 3
Proc 4 = Number of procedures on Day 4
C Age = Child’s age
LOS = Length of stay
B Order = Birth order
Educ= Education level of parents
M Age = Mother’s age
F Age = Father’s age (r)
1. Alzawad, Z. Lewis, F. M., & Walker, A. (2022). Parents’ challenges beyond the pediatric intensive care unit: Fraying at the seams while balancing between two worlds, home and hospital. Children, 9, 267-276.
2. Alzawad, Z., Weiss, J M., Lee, J., Perkhounkova, Y., Hein, M., & McCarthy, A. M. (2024). Exploring factors affecting parental psychological vulnerability during their child’s PICU admission: A prospective pilot cohort study. Journal of Pediatric Health Care, 38(3), 323-336.
3. Debelic, I., Mikolcic, A., Tihomirovic, J., Baric, I., Lendic, D., Niksic, Z., Sencaj B., & Lovric, R. (2022). Stressful experiences of parents in the pediatric intensive care unit: Searching for the most intensive PICU stressors. International Journal of Environmental Research and Public Health, 19(18), 11450-11474.
4. Youngblut, J. M., & Lauzon, S. (1995). Family functioning following PICU hospitalization. Issues in Comprehensive Pediatric Nursing, 18(1), 11-25.
5. Logan, G. E., Sahrmann, J.M., Hongjie, Gu., & Hartman, M. E. (2020). Parental Mental health care after their child’s pediatric intensive care hospitalization. Pediatric Critical Care Medicine, 21 (11); 941 - 948.
6. Toly, V. B., Zauszniewski, J. A., Wang, M., Russell, K. N., Ross, K., & Musil, C. M. (2024). Efficacy of a resourcefulness intervention to enhance the physical and Mental health of parents caring for technology-dependent children at home: A Randomized controlled trial. Journal of Pediatric health Care, 38 93), 337-353.
7. Miles, M. S. et al (1989). A consortium study of parent stressors in the pediatric ICU. Maternal Child Nursing Journal, 18, 181-243.
8. Stremler, R., Haddad, S., Pullenayegum, E., Parshuram, C. (2017). Psychological outcomes in parents of critically ill hospitalized children. Journal of Pediatric Nursing, 34, 36-43.
9. Hagstrom, S. (2017). Family stress in pediatric critical care. Journal of Pediatric Nursing, Nursing Care, Children and Families, 32, 32-40.
10. Tomlinson, P. S., Kirschbaum, M., Harbaugh, B., & Andersen, K. H. (1996). The influence of illness severity and family resources on maternal uncertainty during critical pediatric hospitalization. American. Journal. of Critical Care, 5(2), 140-146.
11. Waller, D.A., Todres, I. D., Cassem, N. H., & Anderton, A. (1979). Coping with poor prognosis in the PICU. The Cassandra Prophecy. American Journal of Disabled Child, 133(11), 1121-1125.
12. La Montagne, L. Hepworth, J. T., Pawlak, R., & Chiafery, M. (1992) Parental coping and activities during pediatric critical care. American Journal of Critical Care, 1(2): 76-80.
13. Schwab, R. (1996). Gender differences in parental grief. Death Studies, 20(2), 103-113.
14. Mirowsky, J., & Ross, C. E. (1995). Sex differences in distress: Real or artifact? American Sociological Review, 60(3), 449-468.
15. Sharkin, B. S. (1993). Anger & gender: Theory, research and implications. Journal Of Counseling and Development, 71(4), 386-389.
16. Dutton, D. G., Webb, A. N., & Ryan, L. (1994). Gender differences in anger/anxiety reactions to witnessing dyadic family conflict. Canadian Journal of Behavioral Sciences, 26(3), 353-364.
17. Kopper, B. A., & Epperson, D. L. (1991). Women and Anger: Sex and Sex Role. Comparisons in the expression of anger. Psychology of Women Quarterly, 15(1), 7-14.
18. Harris, M. B. (1993). How provoking? What makes men and women angry? Aggressive Behaviors, 19(5), 199-211.
19. Harris, M. B. (1993). How provoking? What makes men and women angry? Aggressive Behaviors, 19(5), 199-211.
20. Huckabay, L. M. D., & Tilem-Resnick, D. (1999). A study of parental daily stress levels in PICU in an emergency admission. Dimensions of Critical Care Nursing, 18 (2): 36-42.
21. Barris, B. P. (1999). When Chicken Soup Isn’t Enough: Managing Your Anger in an Increasingly Angry World. Smiling Warthog Publishers.
22. Lazarus, R. S., & Launier, R. (1978). Stress-related transaction between person and environment. In L. A. Previn, & M. Lewis (Ed.), Perspectives in International Psychology. (pp 287—327). Plenum Press. New York.
23. Ellis, A. (1977). Anger: How to Live with and Without, A Citadel Press Book, Carol Publishing Group.
24. Roberts, R. L. (1986). Behavioral Concepts and the Critically Ill Patient. 2nd Ed. Appleton Century Crofts.
25. Zuckerman, M., & Lubin, B. (1985). Manual for the MAACL-R, The Multiple Affect Adjective Check List Revised, San Diego, Calif.: Edits Publishers.
26. Farrell, M. F. & Frost, C. (1992). The most important needs of critically ill children: Parents’ perceptions. Intensive and Critical Care Nursing, 8, 130-139.
27. Munro, R. H. et al, (1986). Statistical Methods for Health Care Research, J. B. Lippincott.
The Roles of Choline in Maintaining Optimal Health
The Effects of Intake of Bread with Treated Corn Bran Inclusion on Postprandial Glyceamic Response
Food Waste throughout the Food Production Continuum – Water Food and Energy Nexus
Use of Lightly Potassium-Enriched Soy Sauce at Home Reduced Urinary Sodium-to-Potassium Ratio
A Different Type of Critical Migration
PRECEDE: A Conceptual Model to Assess Immigrant Health
Walking Together: Supporting Indigenous Student Success in University
Cosmetic Surgery and Body Image in Race/Ethnic Minorities
Our articles most useful
Gina S. Brown, Devora R. Winkfield, Maija Anderson, Payton Gladden
Published : April 03, 2024
Archives of Healthcare
Loucine M. Huckabay
Published : July 31, 2023
Archives of Healthcare
Cathy MacDonald and Lance Bright
Published : February 16, 2023
Archives of Healthcare